Childhood asthma
Children aged ≤ 5 years old
Approach to asthma in this age group are often challenging due to the various other causes that can manifest with similar symptoms as asthma e.g. viral induced wheeze. There is also lack of diagnostic test as objective testing of lung function (e.g. bronchodilator test/air flow variability) are often not feasible.
Diagnosis
Asthma diagnosis in this age group is often based on:
- Symptom patterns – recurrent ep. of wheeze, cough, SOB (often manifested by activity limitation), and nocturnal symptoms/awakening.
- Presence of risk factors – family or personal history of atopy
- Therapeutic response to controller treatment
- Exclusion of other possible diagnosis.
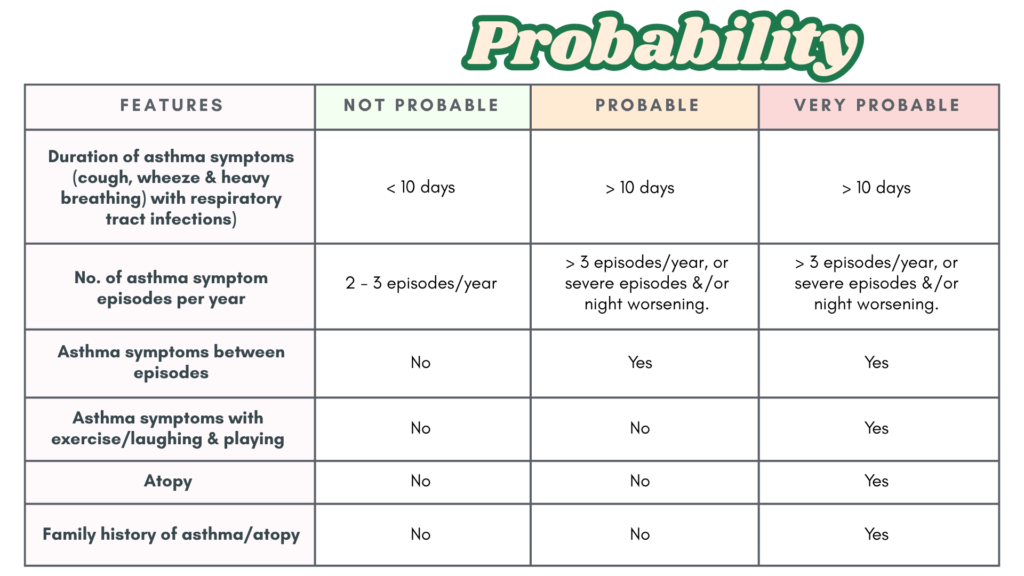
The table below provides guidance on the likelihood of asthma diagnosis.
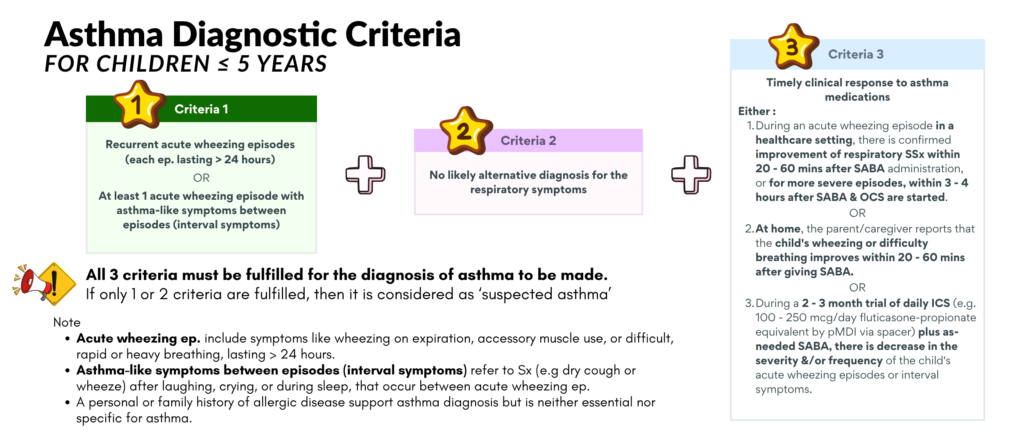
GINA 2026 Diagnostic Criteria
The diagnosis of asthma in children ≤ 5 years old has shifted from probability-based to criteria-based.
All 3 criteria must be met for the diagnosis of asthma in this age group to be made.
Take note that :
1. Wheezing must be confirmed at least once, preferably by,
- Direct observation by a healthcare worker (HCW)
- Video/audio recording verified by HCW
- Reliable parent/care giver that are able to distinguish wheezing vs other sources of noisy breathing. (⚠️ Not all noisy breathing = wheeze)
2. The younger the child, the higher the likelihood of an alternative diagnosis. A 1st episode of wheezing occurring before 12 months of age is more commonly due to bronchiolitis rather than asthma.
3. Further evaluation/investigation is needed TRO alternative diagnosis if any of the following are present :
- Failure to thrive
- Neonatal or very early onset of symptoms (especially if associated with failure to thrive).
- Vomiting associated with respiratory symptoms
- Continuous wheezing, recurrent stridor or seal-like barking cough -> consider airway malacia
- Failure to respond to asthma medications (inhaled ICS, oral steroids or SABA)
- No association of symptoms with typical triggers, such as viral URTI
- Focal lung or cardiovascular signs, or finger clubbing.
- Hypoxemia (< 95%) when awake (outside the context of an exacerbation
Predicting the likelihood of developing atopic asthma.
Several tools have been developed to identify which wheezing children ≤ 5 years are at high risk of having asthma symptoms that persist after the preschool years.
3 prediction tools that have been validated include :
- Asthma Predictive Index (from Tuscon, USA)
- Prevention & Incidence of Asthma & Mite Allergy (PIAMA index, from the Netherlands)
- Leicester tool (from UK)
However, these tools have poor predictive accuracy, with variation in sensitivity & positive predictive value.
A positive family history of allergic disease or evidence of atopy in children with recurrent wheeze increases the likelihood of developing atopic asthma.
modified Asthma Predictive Index (mAPI)
Major criteria
- Parental history of asthma (diagnosed by a physician)
- Atopic eczema (diagnosed by a physician)
- Aeroallergen sensitization
Minor criteria
- Eosinophilia ≥ 4%
- Wheezing unrelated to colds (reported by parents)
- Allergic sensitization to food, i.e. milk, egg, peanuts
Risk can be assessed using the modified Asthma Predictive Index (mAPI), which requires ≥4 wheezing episodes per year plus ≥1 major or ≥2 minor criteria.
Assessment
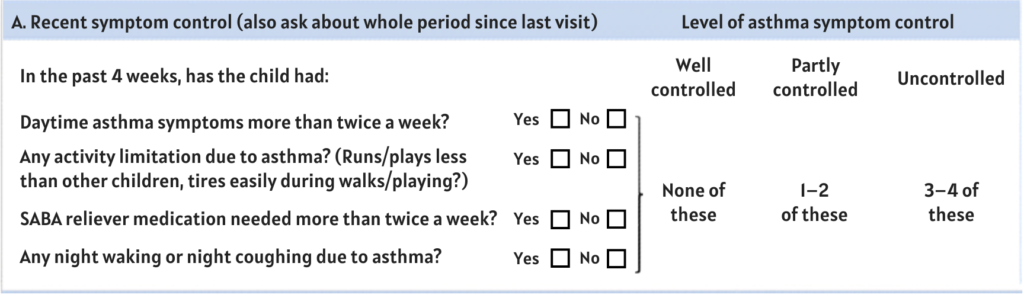
The child should be assessed as that in adults on i) asthma symptom control & ii) future risk for poor asthma outcomes.
Asthma symptom control
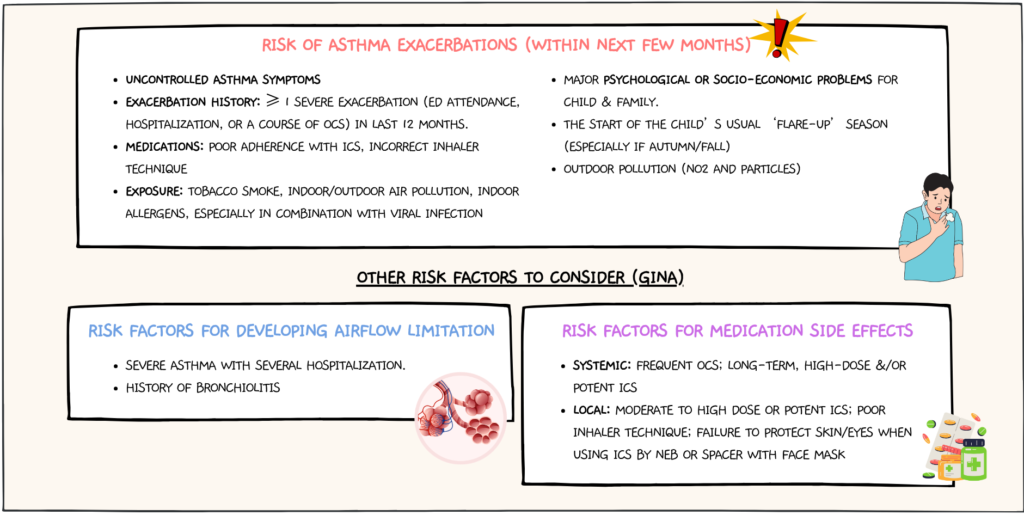
Future risk for poor asthma outcomes.
Investigations
Objective assessment (lung function tests) is difficult to perform in children ≤ 5 years as they are usually unable to perform repeatable expiratory maneuvers.
Alternative measures for lung function testing that may be used in young children include :
a) Oscillometry
- A non-invasive effort-independent lung function test obtained during quiet tidal breathing.
- Suitable for children ≥ 3 years old, & can be used to assess bronchodilator responsiveness.
- As results may vary between devices, device-specific reference values should be used.
b) Bronchial provocation testing
- May be considered in selected cases.
- Should only be done by trained personnel.
Adjuncts that can be done to support the diagnosis of asthma:
i. Chest X-ray – mainly to rule out alternate diagnosis (especially when red flags are present) like:
- Structural airway abnormalities – congenital lobar hyperinflation, vascular ring
- Chronic infections – pulmonary tuberculosis
- Chronic suppurative lung disease or bronchiectasis
- Inhaled foreign body
- Others
ii. Allergic sensitization tests – skin prick testing or allergen-specific immunoglobulin E tests.
- Allergic sensitization is the best predictor for persistent asthma.
- Nevertheless, the absence of sensitization to common aeroallergens does not rule out asthma.
Management
The goals of asthma management are similar to that of the older age groups :
- To achieve good, long-term symptom control
- Maintain normal activities
- To reduce future risks of exacerbation, impaired lung function & development
- To reduce risk of medication side effects.
Interactive diagnostic & management pathway based on the probability of asthma
Childhood Asthma (≤5 years)
Interactive diagnostic pathway for primary care: assess, classify, treat, review, and escalate when needed.
Step 1 — Clinical Assessment
Start with a detailed history and physical examination in a child with recurrent wheeze.
Treatment
Reliever therapy: inhaled SABA (pMDI salbutamol) PRN
Controller therapy:
- Daily low-dose ICS is preferred as the initial treatment. ICS should be given for at least 2 – 3 months to establish it effectiveness.
- Alternative – Montelukast (leukotriene receptor antagonist); caution regarding neuropsychiatric side effects.
There is insufficient data on the safety & effectiveness of ICS/LABA combination in < 4 years old
Inhaler devices of choice: pMDI + spacer with facemask.
ICS dosage in ≤ 5 years old
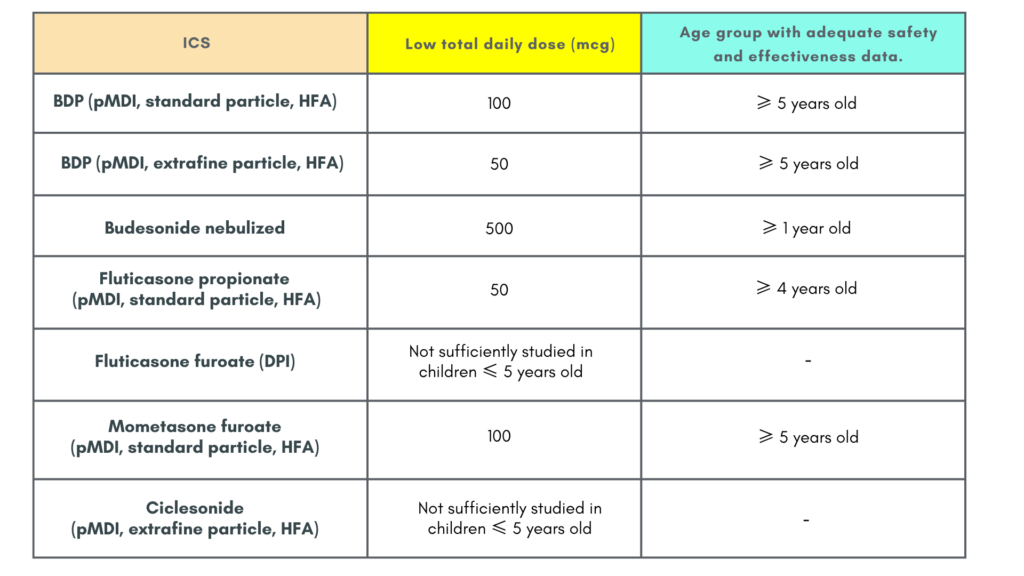
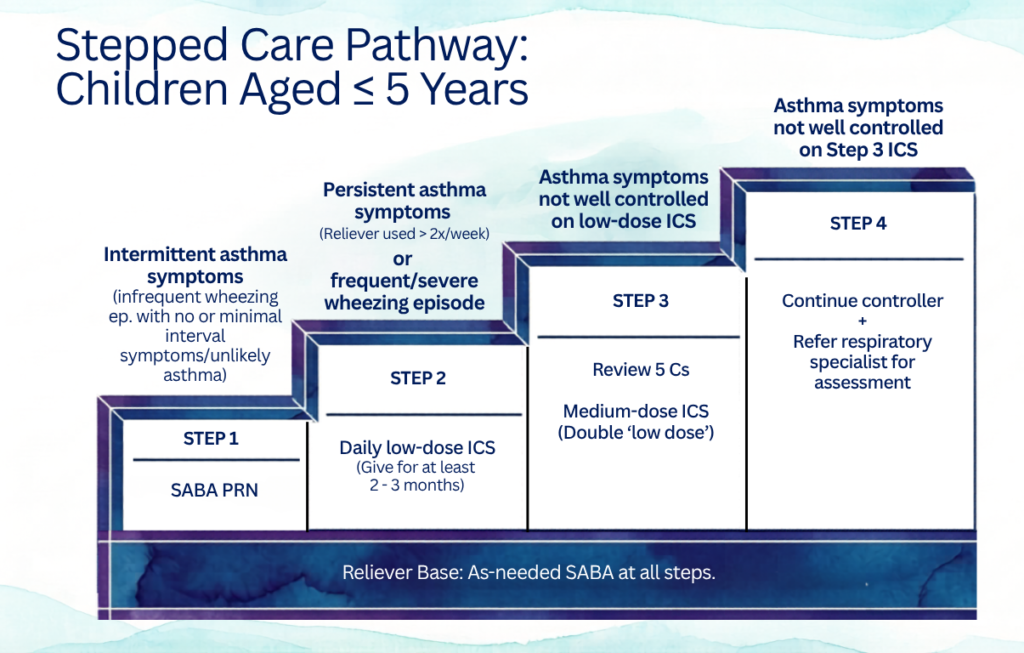
Alternative options for
Step 1 : Consider intermittent short course ICS at onset of viral illness – for those with intermittent viral-induced asthma & no interval symptoms, especially those with underlying atopy, in whom does not respond to inhaled SABA sufficiently.
Step 2 : Daily LTRA or intermittent short course of ICS at onset of respiratory illness.
Step 3 : Consider referral for expert assessment
Regarding pMDI with spacer
pMDI + spacer with mouthpiece or facemask is the preferred inhaler system in young children.
- 0 – 3 years : pMDI + spacer with facemask
- 4 – 5 years : pMDI + spacer with mouthpiece
Child should be switch to mouthpiece as soon as they are able to use it.
Administration technique
- Shake salbumatomol (albuterol) inhaler before each puff.
- Give ONE puff at a time
- Encourage child to take 5 – 6 breaths through the spacer after each puff.
Points to note
- Do not fire multiple puffs into the spacer at once -> may reduce drug delivery.
- Start inhalation ASAP after each actuation (puff). Delay > 30 seconds between puff & inhalation may reduce or increase the amount of drug available..
- When using facemask, ensure that it is well-fitted to minimize drug loss & reduce eye exposure. Clean the skin around nose & mouth after use.
Spacer maintenance.
Plastic spacers may accumulate static electricity which can attract drug particles thus reducing drug delivery.
Static can be reduced by washing it with detergent (do not rinse) & allow it to air dry. Nevertheless, static may re-accumulate over time.
Follow up
Monitoring of symptoms in this age group are mainly based on:
- Clinical symptoms
- Childhood asthma control test (C-ACT)
- Asthma exacerbations
- Inflammatory markers – FeNO
Lung function tests are often not feasible as a tool to monitor their symptoms control.
Assessment at every visit should include :
- Asthma symptom control
- Treatment adherence & inhaler technique
- Risk factors for exacerbation & medication side effects
Important points to note :
1. Growth monitoring – Measure child’s height at least yearly or more often if clinically indicated.
2. Reassessing need for ongoing treatment.
- In children ≤ 5 years, asthma-like symptoms may remit in a substantial portion of them., thus the need for continue controlled therapy should be reviewed regularly.
- Suggest review interval : every 3 – 6 months.
3. Stepping down therapy
- If asthma is well controlled, consider stepping down or discontinuing treatment.
- After step down, review again in 3 – 6 weeks to check for symptom recurrence KIV to restart or stepped up treatment.
Growth & ICS
A small reduction in growth velocity may occur in prepubertal children, particularly during the first 1 – 2 years of treatment.
Long-term impact :
- Effect is generally not progressive or cumulative.
- Long-term studies suggest minimal impact on adult height, only approximately 0.7% difference in final adult height.
⚠️ Poorly controlled asthma itself can impair growth.
Practical principle : Since growth effects are dose dependent, use the lowest effective ICS dose for each child.
References
- Malaysian Thoracic Society, Academy of Medicine of Malaysia, & Lung Foundation of Malaysia. (2014). Clinical practice guidelines: Management of childhood asthma.
- Global Initiative for Asthma. (2024). Global strategy for asthma management and prevention (2024 update)