Childhood asthma

Childhood asthma
This post outlines stable asthma management in two groups: children aged 6–11 years and those ≤5 years. Management of acute exacerbations will be covered in a separate post to ensure clarity and focus.
Please note that the section on children aged 6–11 years (first page) is still based on the Malaysian CPG and GINA 2024 guidelines and will be revised soon in line with GINA 2026 updates. The section for children ≤5 years has already been updated according to GINA 2026 guidance.
Children aged 6 – 11 years
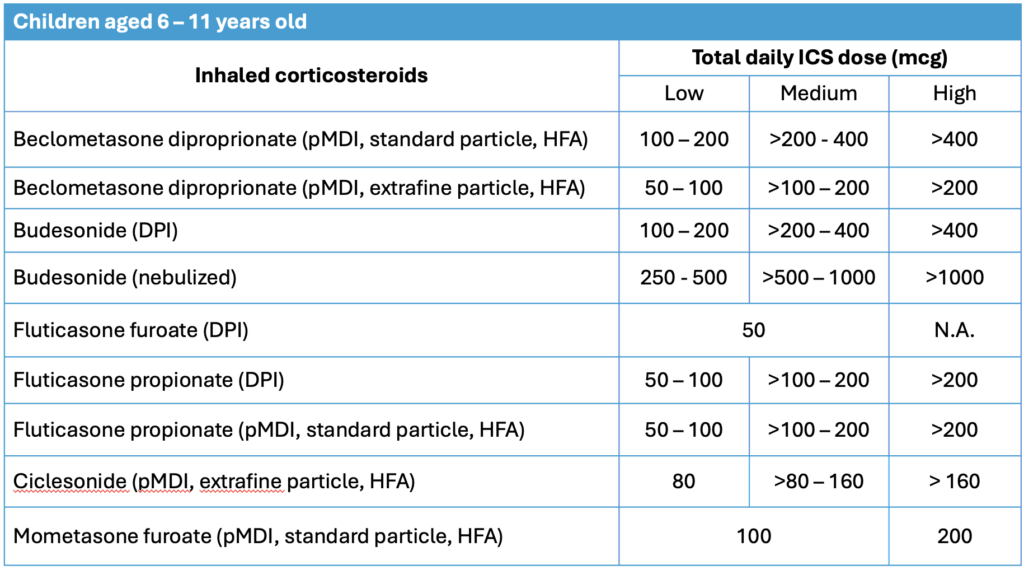
Approach to asthma in this age group is very similar to that of adolescent and adults, with the main difference being ICS dosing.
Typical symptoms
- Recurrent cough (especially nocturnal), wheeze, shortness of breath, or chest tightness
- Often triggered by infections, allergens, or exercise
Supportive features
Atopy in the child or family supports the diagnosis:
- Eczema
- Allergic rhinitis
- Conjunctivitis
Less suggestive of asthma: Chronic cough without wheeze → consider other causes.
Diagnosis
Objective lung function testing can usually be performed in this age group, and these include:
a) Bronchodilator reversibility test
- Positive if FEV1 improves ≥ 12% or PEFR by ≥ 15% after bronchodilator.
b) Other objective measurements:
- ≥ 12% improvement in FEV1 after 4 weeks of ICS.
- ≥ 12% reduction in FEV1 in exercise challenge test
- ≥ 15% reduction in FEV1 in bronchial hyperresponsive challenge test
- Significant diurnal variability (≥ 15%) of PEFR
Other supportive tests:
- Fractional exhaled Nitric Oxide (FeNO): raised level supports eosinophilic airway inflammation, but is not diagnostic on its own
- Allergy test: positive skin prick test to aeroallergens supports the likelihood of asthma.
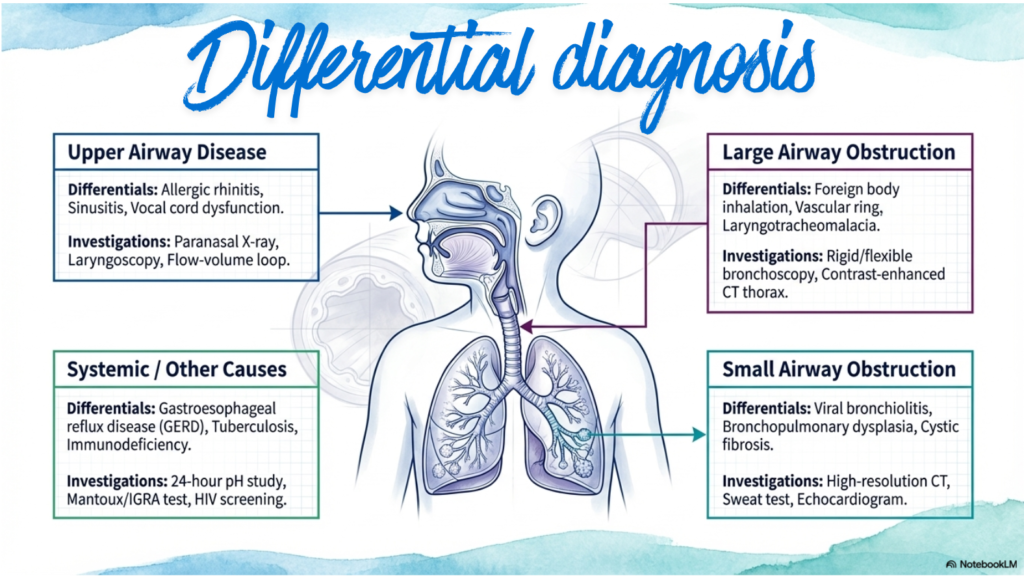
Differential diagnosis
Can be generally divided into upper airway disease, large airway obstruction, small airway obstruction or systemic/other causes.
Severity assessment
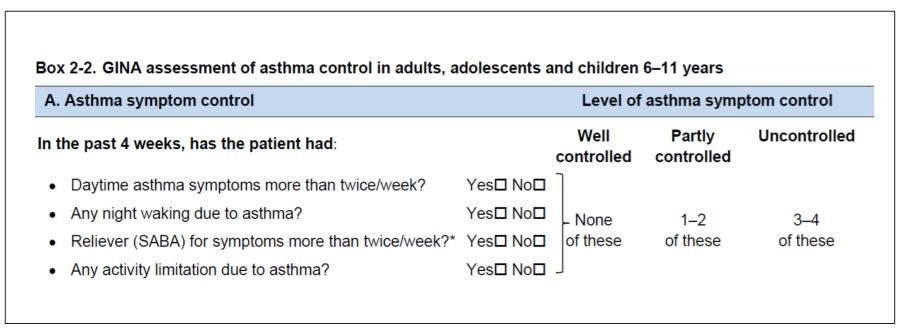
Once the diagnosis is ascertained, the next step is to assess the severity (similar to that in adolescent and adult patients)
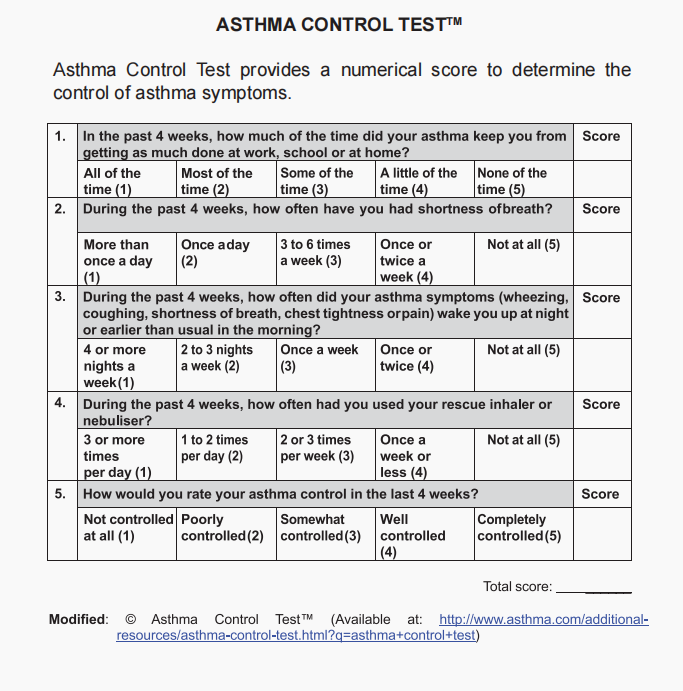
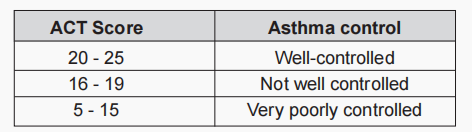
The GINA questionnaire & Asthma Control Test can both be used.
GINA questionnaire
Asthma Control Test
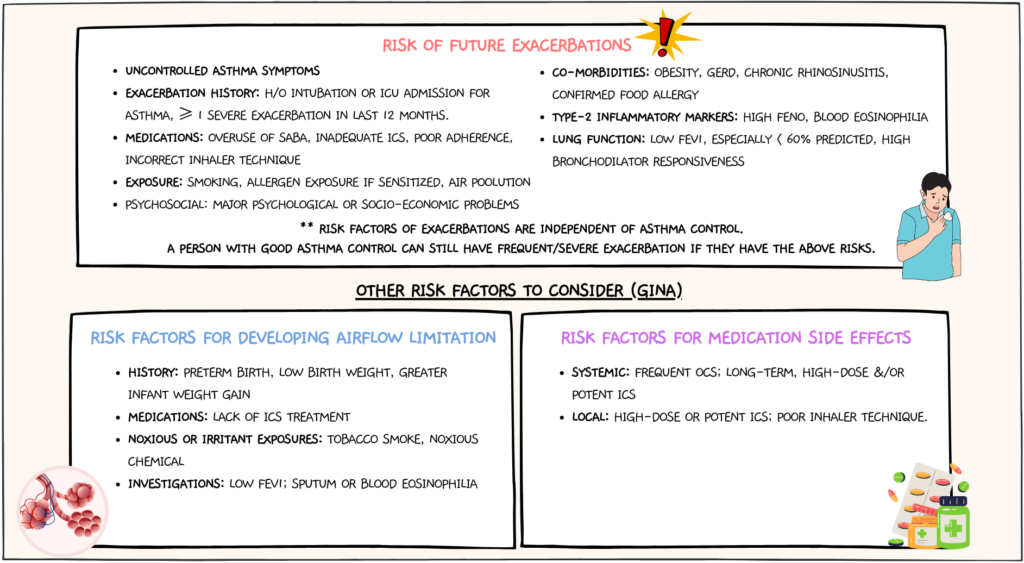
Risk factors for poor asthma outcomes should also be assessed & these include risk factors for exacerbations, risk factors for developing persistent airflow limitation, & risk factors for medication side effects.
Management plan
Consists of :
- Patient &/or parental education
- Prevention & risk reduction of asthma flare-ups
- Pharmacotherapy
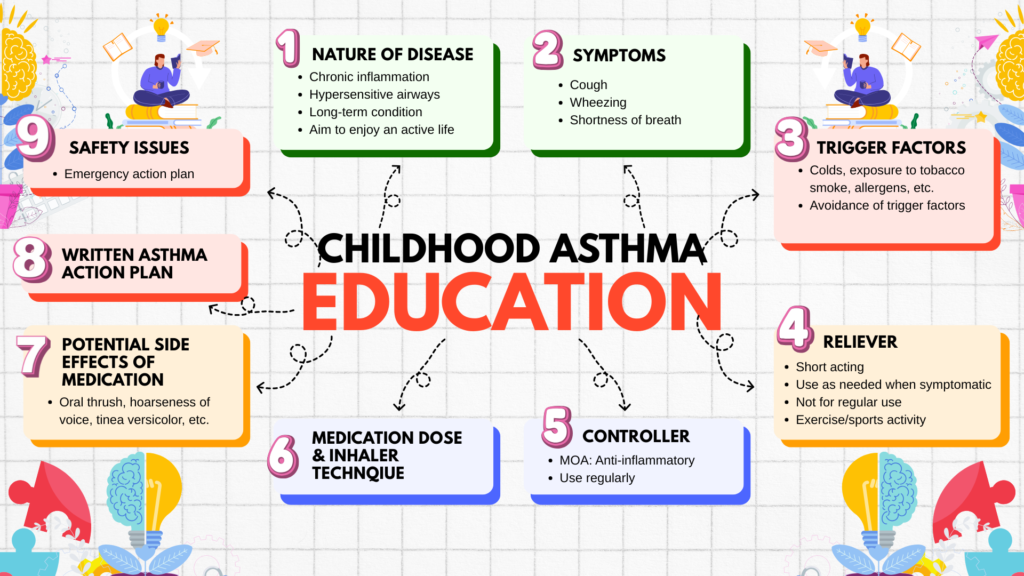
Patient &/or parental education
Prevention & risk reduction of asthma flare-ups
These include:
- Avoidant of tobacco smoke & air pollutants.
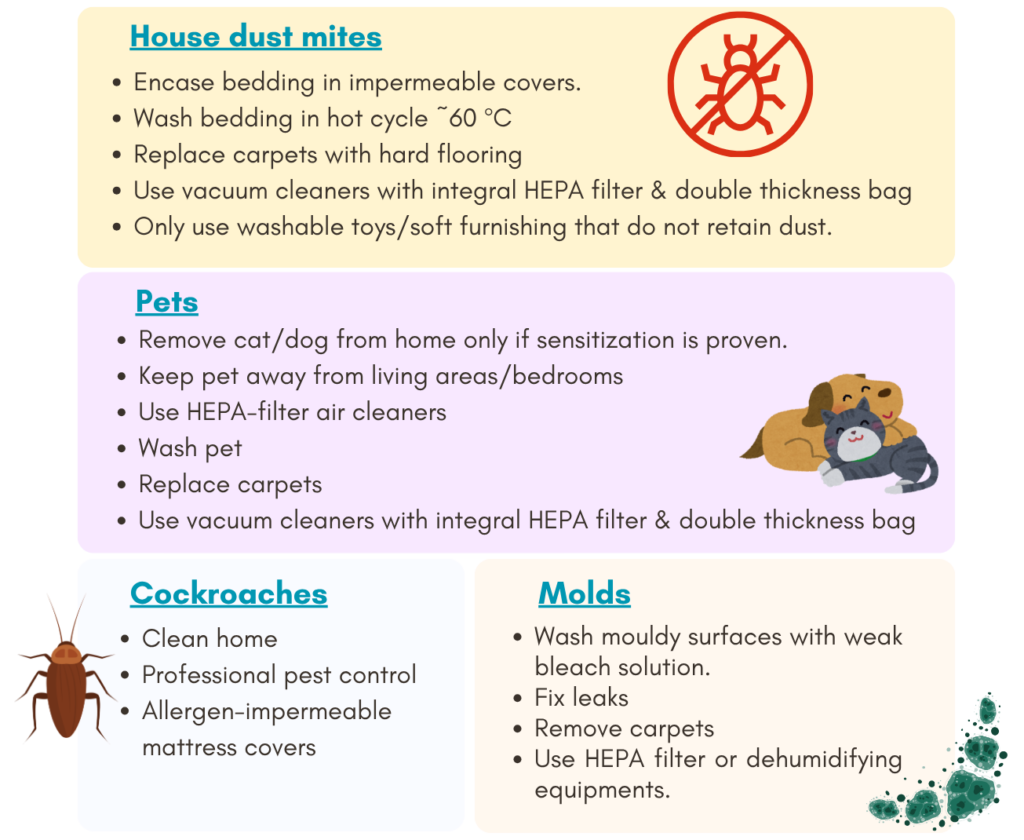
- Reduction of environmental allergens (indoor & outdoor) exposure.
- Vaccinations & good hand hygiene to reduce risk of respiratory tract infection.
Pharmacotherapy
Consist of 2 components: Reliever & Controller therapy
a) Reliever therapy
Aim: To relieve acute asthma symptoms.
Inhaled Short-acting β2 agonist (SABA) is the drug of choice,
- may be used alone OR
- in combination with ICS (e.g. as-needed ICS formoterol or as-needed ICS-SABA).
b) Controller therapy
Aim: For prevention of asthma symptoms
ICS-containing medications remain the anti-inflammatory treatment of choice.
Inhaler devices recommended:
- pMDI + spacer with mouthpiece (preferred)
- pMDI + spacer with facemask
- Dry powder inhaler (if the child has sufficient inspiratory flow)
- Breath-actuated inhaler (> 7 years)
Starting pharmacotherapy should be based on symptoms severity.
In contrast to adolescent and adults, there is only 1 track for managing stable asthma in this age group of 6 – 11 years, as shown below.
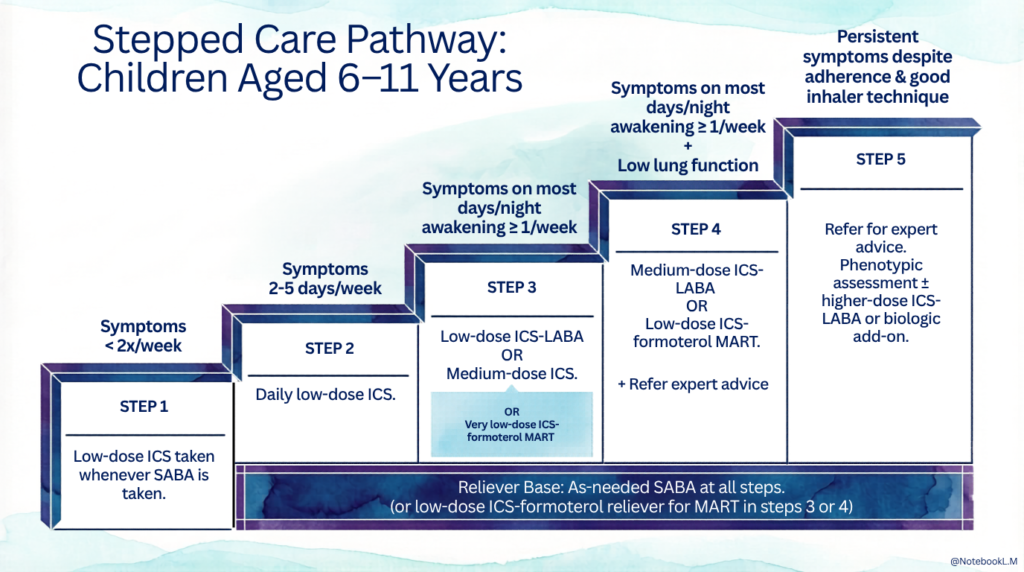
Alternative options for
Step 2 : Daily LTRA or low-dose ICS taken whenever SABA taken
Step 3 : Low dose ICS + LTRA
Step 4 : Add tiotropium or add LTRA
Step 5 : As a final option, consider administering a low-dose OCS. However, it is crucial to consider the potential side effects of OCS and refer the patient to a specialist if they have not already done so.
Follow up
1. Asthma control should be assessed in 4 – 8 weeks after starting controller, and every 3 – 12 months thereafter.
Tools that can be used for asthma monitoring include:
a) Clinical
- Clinical symptoms
- Childhood asthma control test (C-ACT)
- Asthma Control Questionnaire (ACQ)
- Asthma exacerbations
- Asthma Quality of Life Questionnaire (QoLQ)
b) Lung function tests: PEF, bronchodilator response
c) Bronchial hyperresponsiveness: Exercise
d) Inflammatory markers: FeNO
2. Stepwise medication – step-up/step-down controller medication accordingly
A short-term increase in maintenance ICS dose for 1 – 2 weeks may be needed during viral infections or seasonal allergen exposure.
A sustained step-up in treatment may be recommended after confirming symptoms are attributed to asthma, ensuring proper inhaler technique and adherence, and addressing modifiable risk factors.
Consider stepping down treatment only if asthma control is achieved for at least 3 months.
- ICS should be adjusted to the minimum dose required to maintain asthma control.
- Do not step down too rapidly as it can increase the risk of exacerbations.
- Feasible approach: Gradual reduction in ICS doses by 25 – 50% every 3 months.
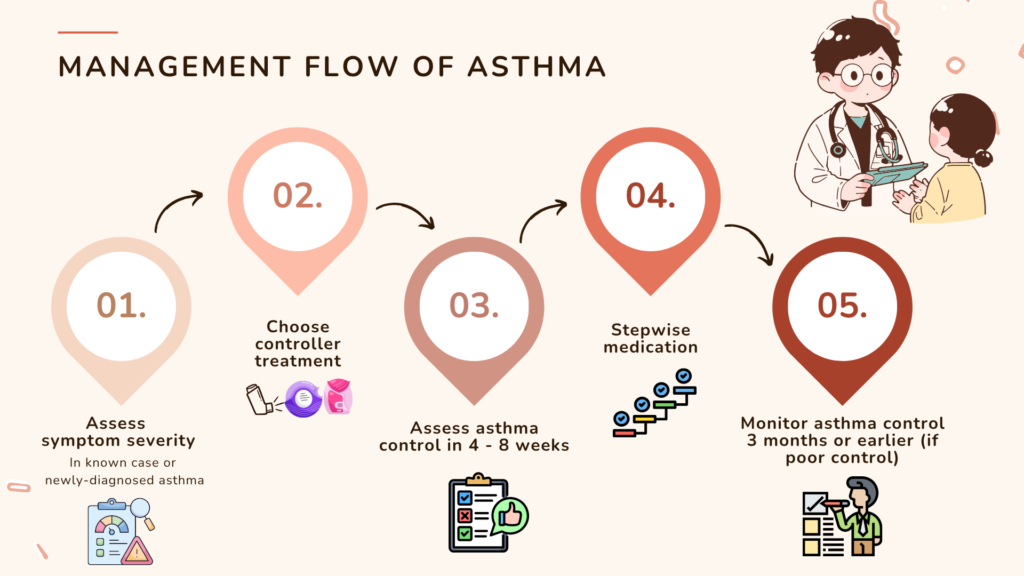
Summarized approach to asthma management
Difficult-to-treat vs Severe asthma
Difficult-to-treat asthma
Definition: Persistent symptoms &/or frequent asthma attacks despite on high dose controller treatment (i.e. GINA steps 4 or 5).
May be due to modifiable factors like :
- Incorrect diagnosis
- Incorrect inhaler technique
- Poor adherence
- Presence of comorbidities & contributory factors
- Persistent exposure to allergens

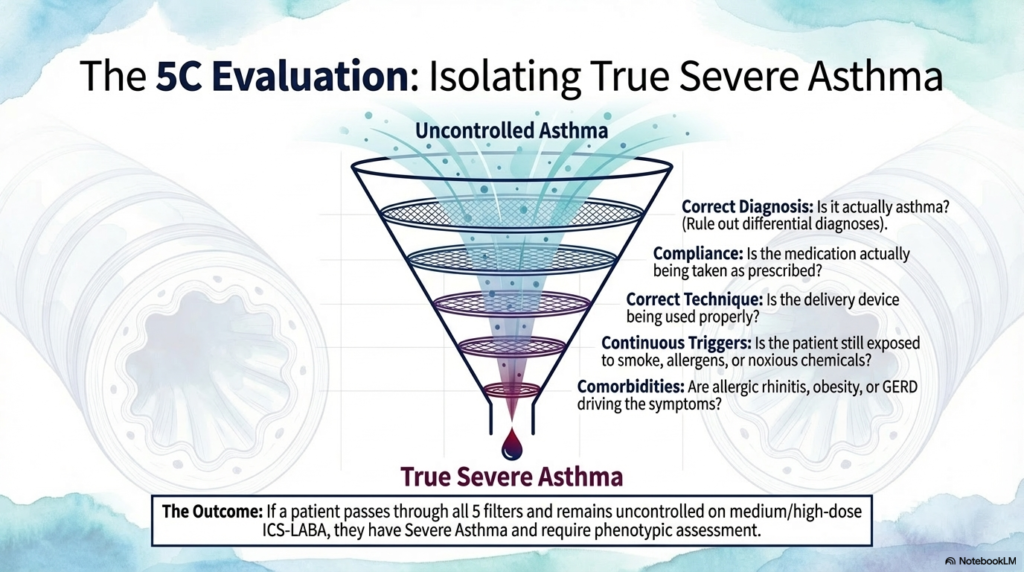
The 5C evaluation is thus important especially in patients who appear difficult-to-treat, as it ensure that we addresses the possibility of the modifiable factors.
The 5Cs:
- Correct diagnosis of asthma.
- Compliance evaluation
- Correct inhaler technique
- Continuous exposure to triggers
- Comorbidities & contributing factors assessment.
Severe asthma
If all the modifiable factors have been addressed and symptoms still remained uncontrolled despite high-dose ICS-LARA or asthma that worsens when high-dose treatment is decreased, then it is termed as severe asthma.
Having one or both of the criteria below qualifies patient as having uncontrolled severe asthma :
- Poor symptom control (frequent symptoms or reliever use, activity limited by asthma, night waking due to asthma)
- Frequent exacerbations (≥ 2/year) requiring OCS, or serious exacerbations (≥ 1/year) requiring hospitalization.
These group of patients should be referred for specialist assessment as they will likely require phenotypic assessment to decide on biological therapy.