Frailty
Frailty
Definition
Frailty is defined by the International Association & Gerontology and Geriatrics Frailty Consensus as :
“A reduced strength & physiologic malfunctioning that increases an individual’s susceptibility to increased dependence, vulnerability, & death”
It is more prevalent among females & its prevalence increases with age.
However, frailty is not an inevitable consequence of aging, as many adults reach advanced ages without developing frailty.
Frailty can be a useful marker of adverse outcome & is increasingly used across specialties such as oncology, cardiology & orthopedics to predict outcomes in older patients.
Etiologic factors for frailty may include :
- Physiological changes &/or diseases associated with aging.
- Inflammation
- Sarcopenia
- Polypharmacy
- Endocrine disorders
- Protein energy malnutrition
- Social isolation
- Povery.
Frailty as a spectrum
Conceptually, it exists along a continuum ranging from robust, pre-frail, to frail.
It is a dynamic entity where an individual can transition between states (based on stressors & interventions), e.g.
- Hospitalization (stressor) may accelerate decline & result in progression from robust to frail.
- Regular physical activity (intervention) can help prevent, delay, or reverse its development (at least partially), particularly in the early stages.
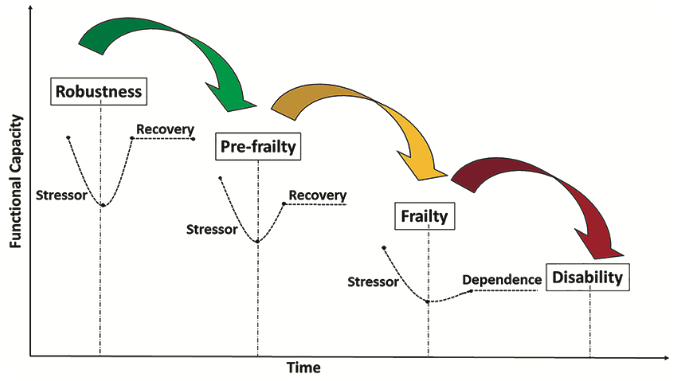
The cascade of functional decline in older adults from independence, through to frailty and disability (in the absence of intervention) [Based on concepts and findings by Dapp et al. Hoogendijk et al. , Clegg et al. and Fried et al.
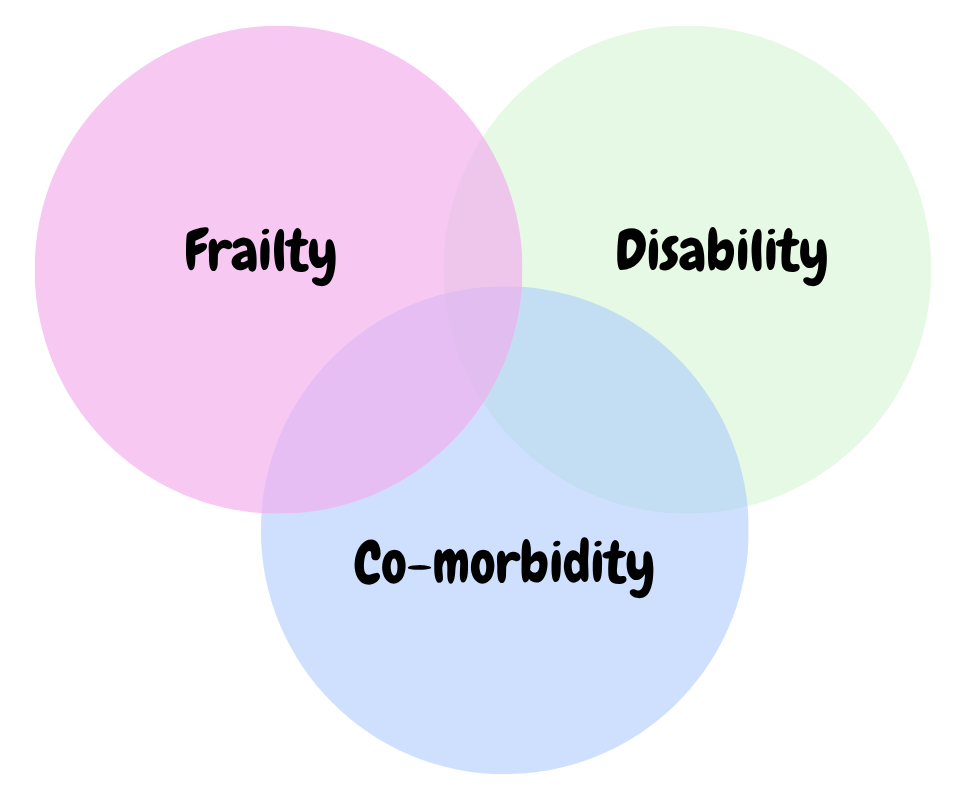
Frailty – Comorbidity – Disability
Frailty may occur independently of comorbidity, and while it is causally associated with disability, it is not synonymous with disability.
An individual may be :
- Frail without significant comorbidity or impairment in activities of daily living (ADLs);
- Living with multiple comorbidities without being frail; OR
- Disabled without meeting criteria for frailty
3 major approaches to define frailty
1. The Physical Phenotype Model (Fried et al.)
This model sees frailty as a distinct clinical syndrome (“phenotype”) caused by physiological dysregulation in energy & complex adaptive systems essential to homeostasis.
Frailty is identified by the presence of at least 3 of the following 5 signs:
- Weakness (reduced grip strength)
- Slower walking speed
- Unintentional weight loss
- Feeling easily exhausted
- Low physical activity
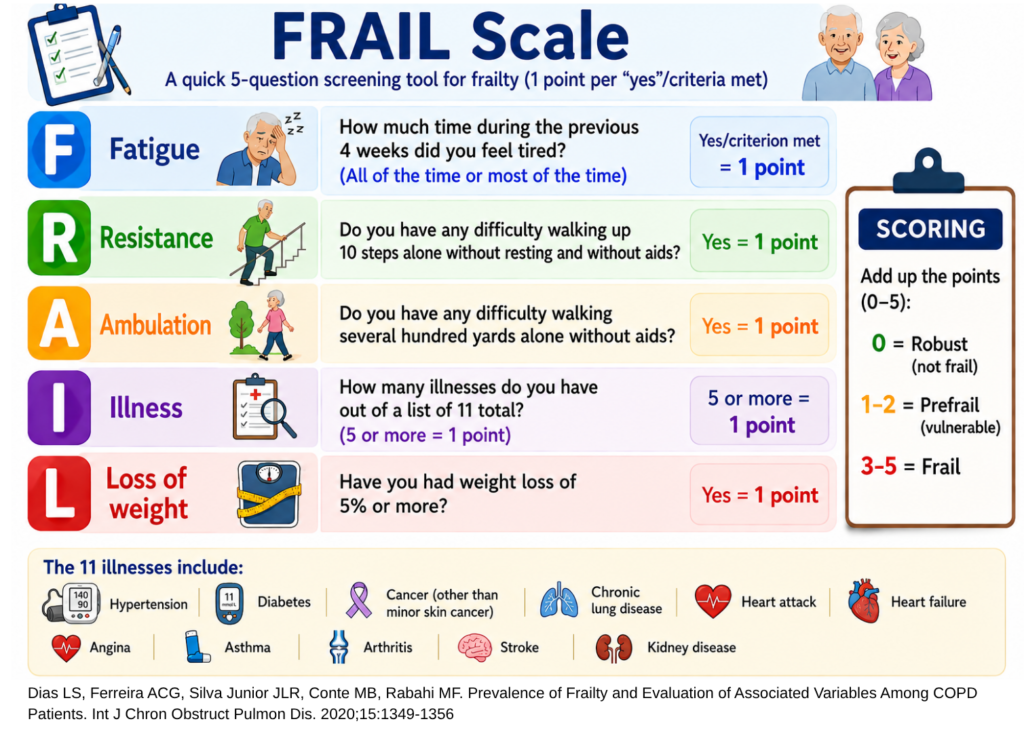
A rapid screening tool derived from this model is the FRAIL scale.
2. The Deficit Accumulation Model (Rockwood & Mitnitski) which captures multimorbidity
This model defines frailty as a dynamic state resulting from the accumulation of various health deficits (e.g. symptoms, disease, disabilities, or laboratory abnormalities).
It identifies frailty by using the Frailty Index (FI), which is the ratio of deficits an individual has out of a predetermined list of 30 or more variables.
FI = Number of deficits present / Total number of deficits assessed.
The Frailty Index reflects biological rather than chronological ageing and provides a quantitative measure of the cumulative burden of multimorbidity.
3. Mixed physical & psychosocial models
These models extend beyond physical impairment to encompass psychological and social determinants of health.
Examples :
- Tilburg Frailty Indicator (TFI)
- Edmonton Frail Scale (EFS)
Who should be screened?
Frailty screening is recommended for :
- Adults ≥ 70 years (ICSFR guideline recommends starting at age of 65 years) OR
- Those who have unintentional weight loss > 5% of their body weight in the previous year.
Barriers to frailty screening may include :
- Lack of public awareness of frailty
- Difficulties for older persons to access & afford primary care service
- The acceptability of screening to older adults
- Lack of clarity regarding which treatment pathways should follow screening/diagnosis.
- Lack of clear evidence that the benefits of routine screening outweigh its associated costs.
Frailty should not be identified solely on the basis of an older person’s appearance, as clinical judgement alone is subject to inter-observer variability.
Instead, validated screening and assessment tools should be used to identify frailty.
Frailty assessment tools
Frailty can be assessed using a range of validated tools, from rapid screening instruments to more comprehensive assessments.
Listed below are some of the validated frailty assessment tools that I think are practical for use in primary care. However, they represent only a small selection of the many available instruments. For a more comprehensive overview, I would highly encouraged you to refer to the Asia-Pacific Clinical Practice Guidelines for Frailty.
1. Rapid screening tools
a) FRAIL scale
- A 5 question survey covering Fatigue, Resistance (stairs), Ambulation (walking one block), Illness (more than 5 conditions) and Loss of weight
- Validated for predicting disability & mortality.
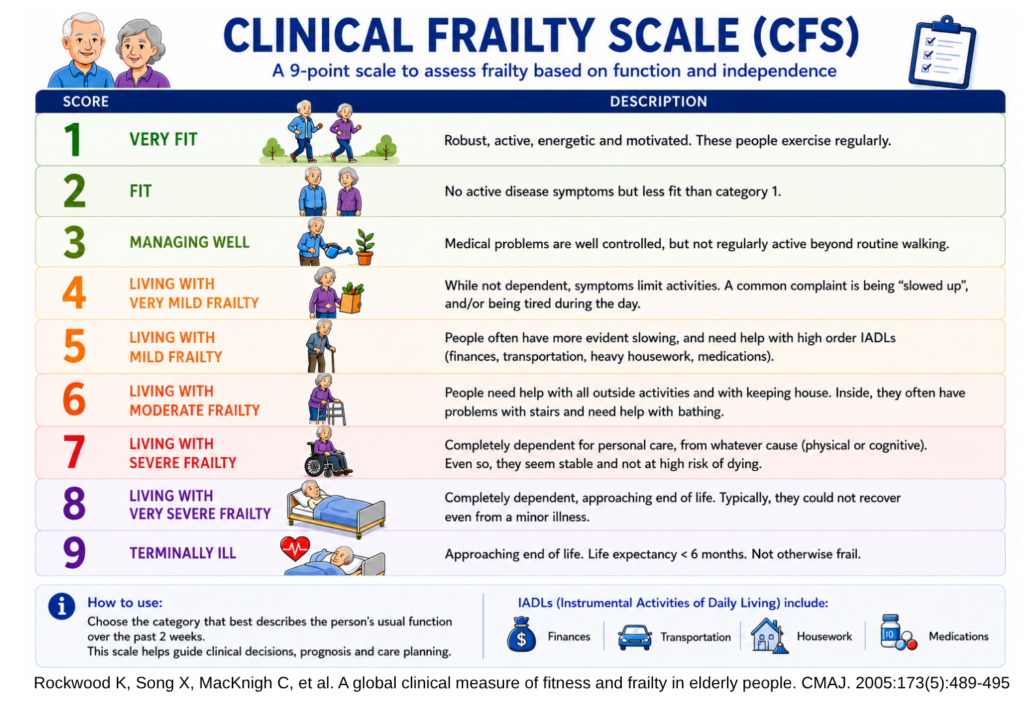
b) Clinical Frailty Scale (CFS)
- A 9 point visual & pictorial scale paired with clinical descriptors ranging from “Very Fit” to “Terminally Ill”.
- Uses clinical judgement to determine an individual’s level of fitness.
A practical shortcut to the Clinical Frailty Scale is to ask whether the patient can go outdoors independently. Patients who are not capable of going outdoors independently are considered frail.
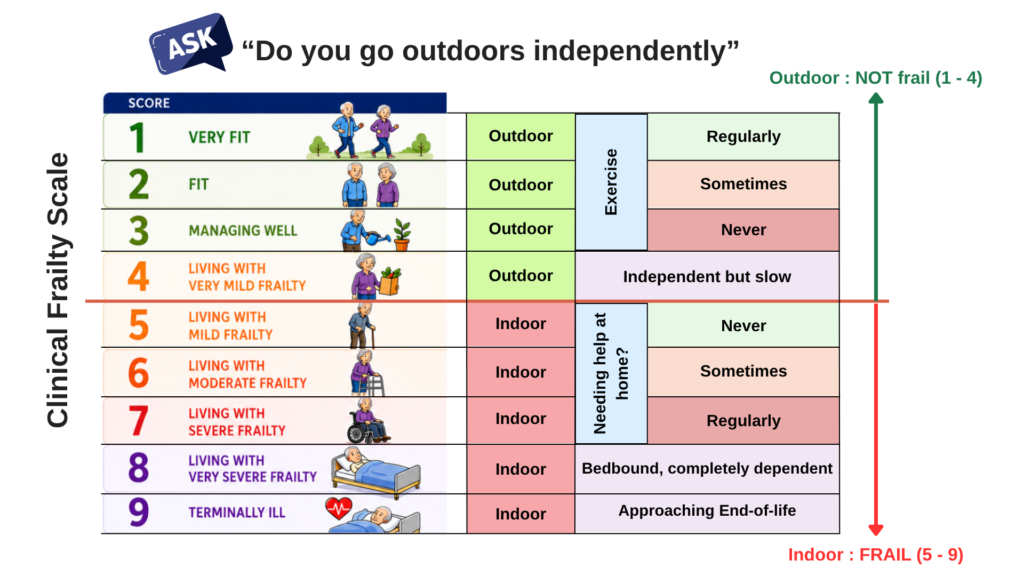
Chong, E., Tham, A., Chew, J., Lim, W. S., Tan, H. N., Ang, H., & Chan, M. (2021). Brief Aids to Guide Clinical Frailty Scale Scoring at the Front Door of Acute Hospitals. Journal of the American Medical Directors Association, 22(5), 1116–1117.e2
2. Physical phenotypes & performance measures
Example : Fried’s Frailty Phenotype (as described above)

Reference : https://frailtyscience.org/simplifying-frailty-assessment-kidney-transplant-patients-introducing-abridged-frailty/
Important considerations :
For performance-based measures, locally defined cut-off values should be used.
E.g. in Asian populations, low grip strength is commonly defined as :
- < 26 kg in men
- < 18 kg in women
- Or the lowest 20th quintile of grip strength
3. Deficit Accumulation Models – Frailty Index (as described above)
4. More Comprehensive & Detailed Assessment Tools
Following a positive frail screen, more comprehensive assessments can help guide individualized management.
These tools include the :
- Edmonton Frailty Scale (EFS)
- Comprehensive Geriatric Assessment (CGA)
Management/Interventions
General principles :
- The perceived benefit of any intervention should outweigh its risks.
- Frailty management should be individualized, as treatment responses may vary according to the patient’s health status, comorbidities, & frailty severity.
- Interventions that are beneficial in the early stages of frailty may be ineffective or even harmful to an older adult with severe frailty.
- Shared-decision making is essential when developing a management plan.
- Healthcare professionals should select interventions that align with – patient preferences & goals, available resources, & minimization of patient harm.
5 key interventions
- Physical activity/Exercise (especially resistance training)
- Addressing polypharmacy
- Screening for reversible causes of fatigue
- Adequate calorie & protein intake
- Vitamin D supplementation – only if deficient (not routinely)
1. Physical activity (Progressive & Individualized + Contains Resistance Training Component) – “Move it, or lose it”
Helps to maintain strength, mobility, function, and independence.
Recommendations :
- Resistance (strength) training is a core component, e.g. dumbbells, resistance bands, weight machines & body-weight exercises.
- Start with multijoint resistant exercise in the initial weeks, then gradually progress to more single-joint exercises as appropriate.
- Balance, aerobic (e.g. walking) and flexibility exercise should also be included as part of a multimodal exercise programme as it has been shown to reduce the risk of major mobility disability in older adults.
Common barriers to exercise may include :
- Fear of falling
- Lack of confidence
- Poor coping strategies
- Social & environmental factors.
2. Addressing polypharmacy
Aim is to reduce medication-related harm by :
- Deprescribing unnecessary medications &
- Adjusting drug doses according to renal function.
Tools that can be used for deprescribing of Inappropriate medications :
a) STOPP/START criteria
- Screening Tool of Older Person’s Prescriptions (STOPP)
- Screening Tool to Alert doctors to Right Treatment (START) criteria
b) The Beers criteria (https://agsjournals.onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.18372)
c) The Mcleod criteria
General deprescribing guidelines are also available. Rather than focusing on specific medications, they emphasize evidence-based decision-making and individual patient preferences. These are:
- The Medication Appropriateness Index (MAI)
- The Inappropriate Medication Use and Prescribing Indicators tool.
Barriers to deprescription may include :
- Incentives to over-prescribe
- Lack of consensus on which medication to deprescrine
- Limited awareness of deprescription benefits
It is the opposite in rural &/or lower socioeconomic areas where the older adults with frailty may have unknown or untreated disease and they lack the resources or necessary medications for treatment.
3. Screen for reversible causes of fatigue (conditional recommendation)
Fatigue is a component of the Fried’s Physical Phenotype.
Screening and treating the reversible causes of fatigue have been found to improve the outcomes of elderly with frailty.
Some of the treatable causes of fatigue include :
- Anemia
- Depression
- Hypothyroidism
- Hypotension
- Vitamin B12 deficiency
- Sleep apnea.
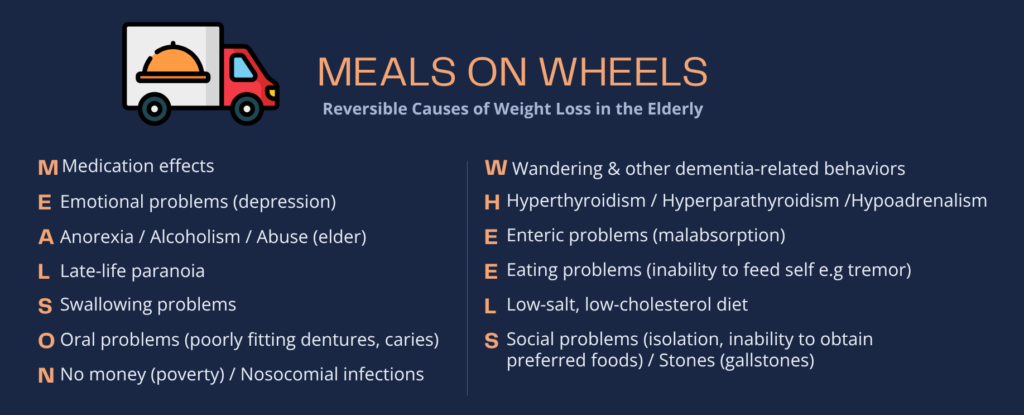
3. Screen for reversible causes of weight loss & consider for protein & caloric supplementation (conditional recommendation)
Weight loss is a key feature of frailty, & reversible causes (Mnemonics – MEALS ON WHEELS) should be screened for & addressed if present.
Protein/caloric supplementation can be considered in frail person with weight loss or malnutrition.
- Assess for weight loss & malnutrition with validated screening tools, e.g. Mini Nutritional Assessment (MNA), its short form version (MNA-SF) or the Malnutrition Universal Screening Tool (MUST).
Essential Amino Acids (EAAs) supplementation may also be beneficial. EAAs are amino acids that cannot be synthesized by the body & must be obtained from the diet.
Recommended protein intake
a) Protein needs with Aging (PROT-AGE) study group recommendation : 0.8 – 1.2 g/kg body weight (BW) per day.
b) European Society for Clinical Nutrition & Metabolism (ESPEN) recommendation :
- At least 1.2 g/kg BW/day for healthy older adults.
- 1.2–1.5 g/kg BW/day for older adults with malnutrition or at risk of malnutrition.
- 0.8–1.0 g/kg BW/day for patients with acute or chronic kidney disease who are not receiving renal replacement therapy.
Important considerations :
- Responses to protein supplementation may differ in Asia-Pacific populations.
- Renal function should be monitored when prescribing high-protein supplementation.
4. Prescribe Vitamin D – ONLY when Vit. D deficiency is present (Not routinely)
Vitamin D deficiency is associated with reduced physical functioning, frailty development, as well as falls & mortality.
In older adults with Vit. D deficiency, supplementation has been shown to reduce the risk of mortality, falls & fractures, though these focuses on older adults without frailty. Further research is needed on the role of Vit. D supplementation in frailty prevention & treatment.
Recommended dose : 800 – 1000 IU daily, adjusted according to the individual’s condition, diet, & sunlight exposure.
Important consideration : High-dose Vit. D supplementation in individuals without deficiency may increase the risk of falls & fractures.
5. Others (addition by the International Conference of Frailty and Sarcopenia Research [ICSFR] task force on frailty)
a) Oral health (Consensus based recommendation, no clinical trials)
- Advise older adults with frailty on the importance of oral health Older adults with frailty are more likely to have edentulism (reduced tooth number) and lower occlusal force (bite strength)
b) Social support (Strong recommendation; very low certainty of evidence)
- Social isolation is a major risk factor for frailty progression.
- Assess & provide social support when needed to :
– Address unmet care needs.
– Improve adherence to management plan.
References
- Dent, E., Lien, C., Lim, W. S., Wong, W. C., Wong, C. H., Ng, T. P., Woo, J., Dong, B., de la Vega, S., Hua Poi, P. J., Kamaruzzaman, S. B. B., Won, C., Chen, L. K., Rockwood, K., Arai, H., Rodriguez-Mañas, L., Cao, L., Cesari, M., Chan, P., Leung, E., … Flicker, L. (2017). The Asia-Pacific Clinical Practice Guidelines for the Management of Frailty. Journal of the American Medical Directors Association, 18(7), 564–575. https://doi.org/10.1016/j.jamda.2017.04.018
- Dent, E., Morley, J. E., Cruz-Jentoft, A. J., Woodhouse, L., Rodríguez-Mañas, L., Fried, L. P., Woo, J., Aprahamian, I., Sanford, A., Lundy, J., Landi, F., Beilby, J., Martin, F. C., Bauer, J. M., Ferrucci, L., Merchant, R. A., Dong, B., Arai, H., Hoogendijk, E. O., Won, C. W., … Vellas, B. (2019). Physical Frailty: ICFSR International Clinical Practice Guidelines for Identification and Management. The journal of nutrition, health & aging, 23(9), 771–787. https://doi.org/10.1007/s12603-019-1273-z
- Morley, J. E., Vellas, B., van Kan, G. A., Anker, S. D., Bauer, J. M., Bernabei, R., Cesari, M., Chumlea, W. C., Doehner, W., Evans, J., Fried, L. P., Guralnik, J. M., Katz, P. R., Malmstrom, T. K., McCarter, R. J., Gutierrez Robledo, L. M., Rockwood, K., von Haehling, S., Vandewoude, M. F., & Walston, J. (2013). Frailty consensus: a call to action. Journal of the American Medical Directors Association, 14(6), 392–397. https://doi.org/10.1016/j.jamda.2013.03.022
- Dias LS, Ferreira ACG, Silva Junior JLR, Conte MB, Rabahi MF. Prevalence of Frailty and Evaluation of Associated Variables Among COPD Patients. Int J Chron Obstruct Pulmon Dis. 2020;15:1349-1356
https://doi.org/10.2147/COPD.S250299 - Chong, E., Tham, A., Chew, J., Lim, W. S., Tan, H. N., Ang, H., & Chan, M. (2021). Brief Aids to Guide Clinical Frailty Scale Scoring at the Front Door of Acute Hospitals. Journal of the American Medical Directors Association, 22(5), 1116–1117.e2. https://doi.org/10.1016/j.jamda.2021.02.005