Vertigo

Vertigo
“Dizziness” is a common presentation to the primary care settings, and it can be generally categorized into 4 categories:
- Vertigo: Spinning sensation – self or environment
- Disequilibrium: Imbalance while walking/standing
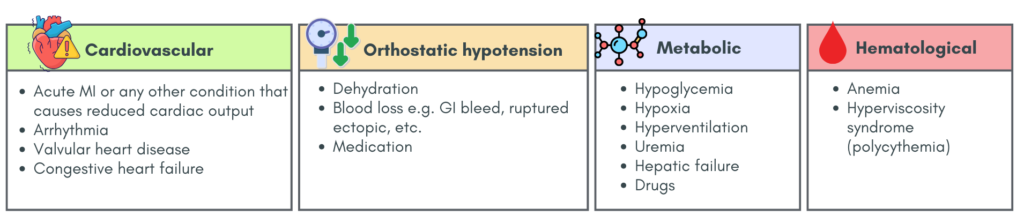
- Light-headedness: Sensation of giddiness
- Pre-syncope: Sensation of feeling faint or about to black out.
In this post, we will primarily discuss vertigo, focusing on the primary care approach, without delving into the comprehensive management of the various causes of vertigo.
Causes
Peripheral causes
- Benign Paroxysmal Positional Vertigo (BPPV)
- Vestibular neuronitis
- Acute Labyrinthitis
- Meniere’s disease
Central causes
- Cerebellar/brainstem stroke
- Tumors, especially cerebellopontine (CP) angle tumor (e.g. brainstem glioma, medulloblastoma & vestibular schwannoma)
- Multiple sclerosis (can also be a peripheral cause)
- Perilymphatic fistule (should be considered if there is a recent history of head injury)
Others
- Psychogenic causes:
– Anxiety attack or panic attack –> hyperventilation –> vertigo
– Stress or trauma - Medications:
– Antidepressants
– Anticonvulsants, e.g. phenytoin
– Antibiotic, e.g. aminoglycosides
– Diuretics
– Salicylates
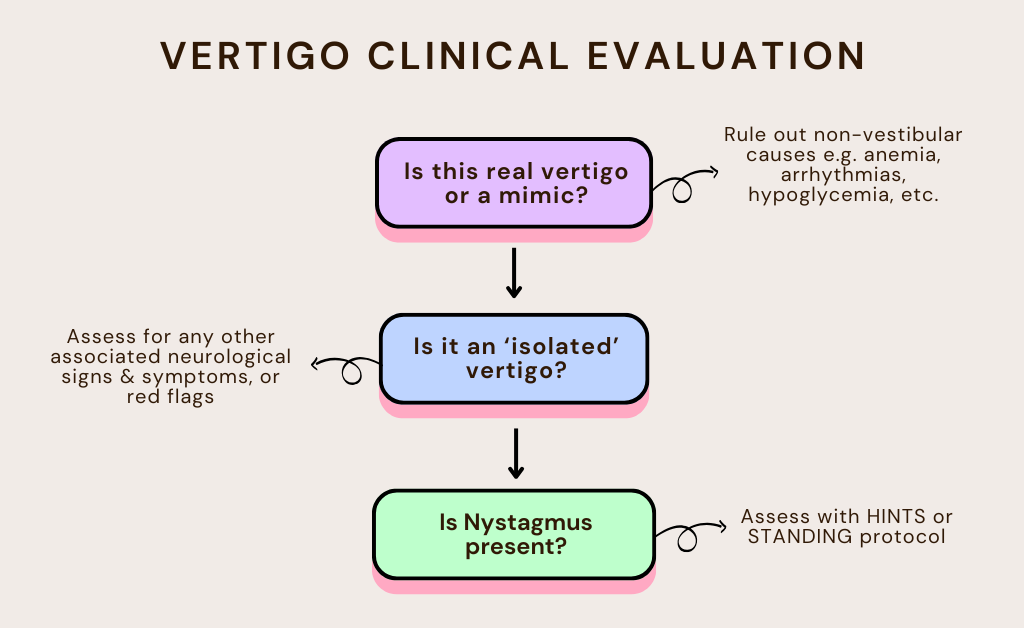
History taking framework
Step 1 – Confirm true vertigo
Ask: “Does it feel like the room is spinning around ?” or “Do you feel like you are the one spinning ?”
Differential diagnosis including other causes of dizziness as mentioned above (“pseudovertigo) & may be:
Step 2 – Distinguish Central vs Peripheral cause (via history)
Using timeline, pattern, associated symptoms & triggering factors
A) Timeline
- Recurrent episode, lasting seconds – minutes –> BPPV
- Solitary episode, lasting minutes – hours –> Vestibular migraine, Transient Ischemic Attack (TIA)
- Episode lasting hours – days –> neuritis, labyrinthitis, CP angle tumors
B) Syndromic pattern
Acute vestibular syndrome
- Sudden onset, continuous vertigo lasting > 24 hours + nausea & vomiting
- Peripheral cause: Vestibular neuritis
- Central cause: Posterior circulation stroke
Episodic vestibular syndrome
- Recurrent, transient ep. of vertigo lasting seconds to hours, with symptom-free intervals.
- Can be:
– Spontaneous, e.g. vestibular migraine, Meniere’s, TIA
– Triggered e.g. BPPV
C) Associated symptoms
- Focal neurological symptoms e.g. diplopia, dysarthria, dysphagia & numbness or weakness point towards central cause.
- Headache, photophobia, visual auras –> vestibular migraine
- Hearing loss & tinnitus –> Meniere’s disease
D) Triggering factors – especially for non-central causes
- Recent history of viral infection –> Acute labyrinthitis, vestibular neuritis
- Medications – anticonvulsants, salicylates, antibiotics
- Change in position of the head –> BPPV
- Loud noises (Tullio phenomenon – vertigo induced by noises) –> commonly seen in semicircular canal dehiscence (SCD)
- Stress or trauma (psychogenic causes)
Physical examination
1. Vital signs – BP, heart rate, SpO2
2. Nystagmus – an integral part of vertigo assessment, if present, can help differentiate between central & peripheral cause.
Steps:
- Determine whether nystagmus is present.
– Spontaneous: nystagmus present while looking at a target in the centre – often points to peripheral cause
– Gaze evoked: ask the patient to hold their gaze about 30 degrees to the right, left, up and down – often points to central pathology - Identify the plane on which the nystagmus beats – horizontal or vertical
- Determine the direction of the nystagmus e.g. right, left, upwards, downwards, rotary, or oblique.
- Additional tests:
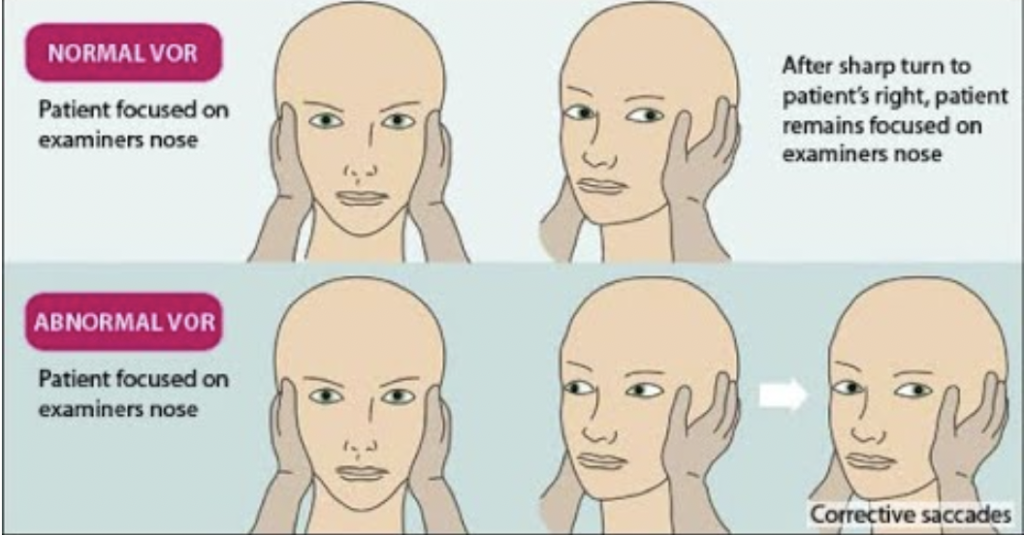
– Head impulse test – if positive = peripheral cause
– Dix-Hallpike – if positive = BPPV
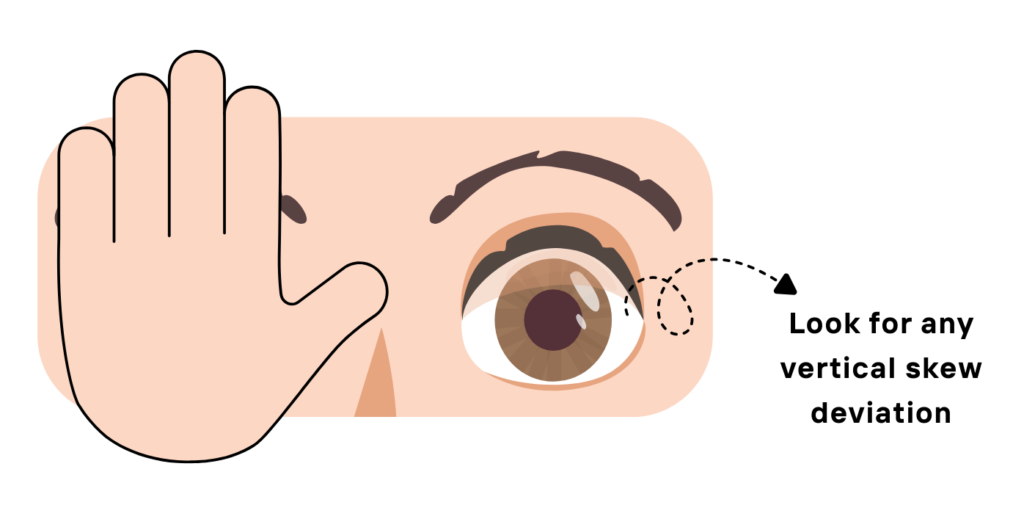
– Cover test – if positive = central cause
Key clinical pearls 💎
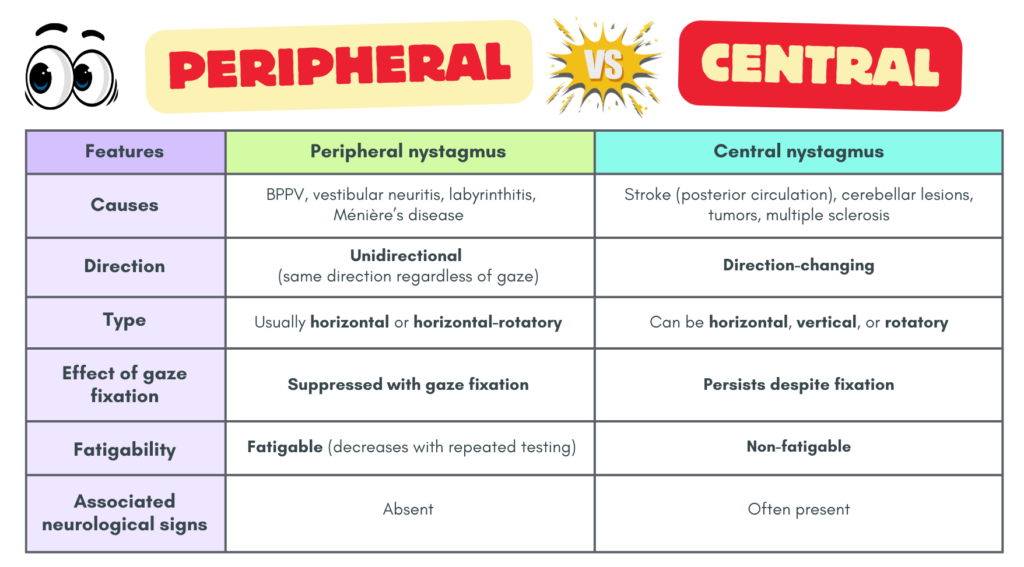
- Vertical nystagmus = central cause until proven otherwise.
- Peripheral nystagmus improves with fixation, while central nystagmus does not.
- Neurological deficits strongly suggest a central lesion.
Structured nystagmus examination – HINTS examination and STANDING protocol
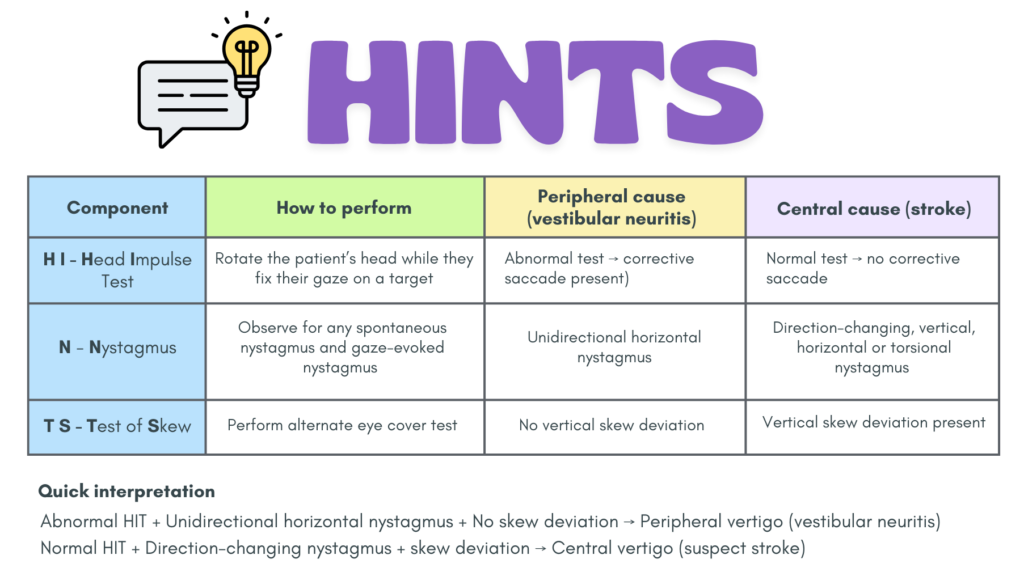
HINTS – Head Impulse, Nystagmus, Test of Skew
Used only for patients who are having a constant “attack” of vertigo that has lasted for hours or days (not transient vertigo)
Can be more sensitive than early MRI for detecting posterior circulation stroke.
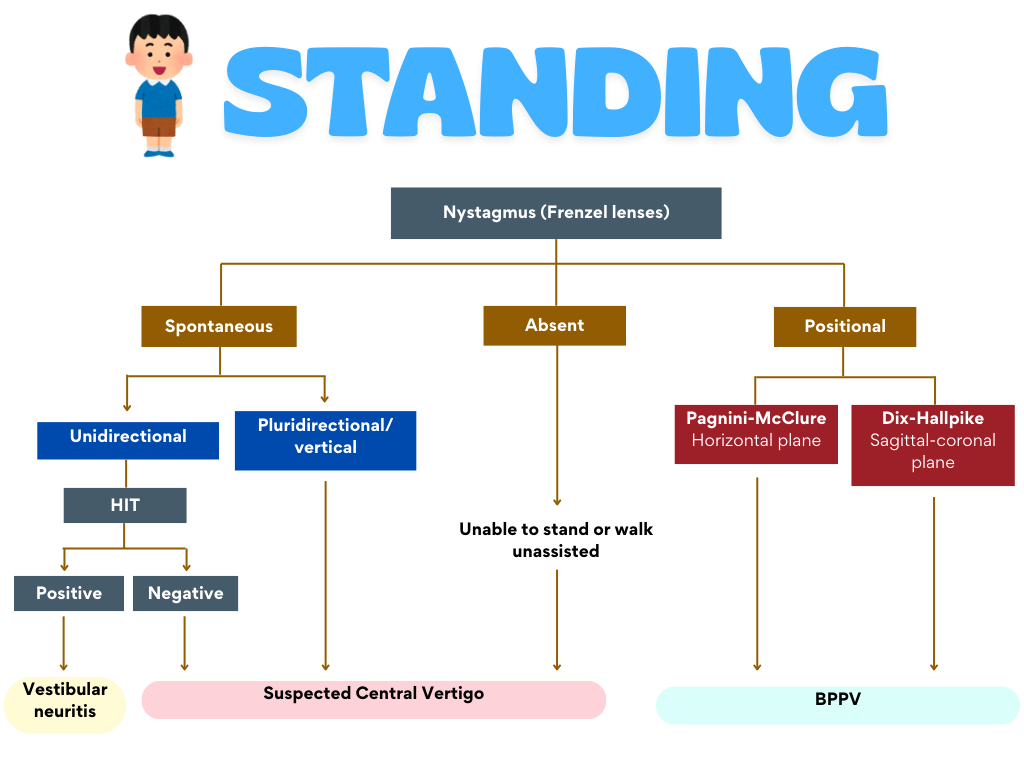
STANDING – SponTAneous nystagmus, Nystagmus Direction, standING
Can be used for patients whose vertigo is constant or whose vertigo is only triggered by movement (in contrast to HINTS which can only be used if the vertigo has lasted for hours – days)
The STANDING protocol also provides an approach to whereby nystagmus is absent.
Other important physical examination
A) Focused neurological examination – including gait, balance, coordination & cerebellar signs
Neurological checklist:
- Language disorders – dysarthria, aphasia
- Ocular motility disorders – nystagmus
- Disorders of the bulbar cranial nerves (glossopharyngeal nerve & vagus nerve)
- Horner syndrome
- Visual field defects
- Motor &/or sensory (tactile, pain & deep) deficits
- Cerebellar signs
- Babinski sign
B) Ear (otoscopic) examination
- Visualize the TM for any vesicles (herpes zoster)/signs of infection/retraction pockets (cholesteatoma)
- Vertigo triggered by pushing on the tragus or with Valsalva maneuver is seen in perilymphatic fistula.
- Hearing assessment should be performed
C) Cardiovascular examination – pulse, BP, heart rate, rhythm, carotid bruits
D) Special test (as mentioned above):
- Dix-Hallpike maneuver
- Head impulse test
Signs that should prompt further assessment includes:
- Depressed consciousness, internuclear ophthalmoplegia, cranial nerve deficits, muscle weakness, hyperesthesia, ataxia, and last but not least, cardiac signs (e.g. murmurs, irregular heartbeats, tachycardia or bradycardia)
Summarized approach
Investigations
STAT capillary glucose should be considered & must be done for all diabetics.
Consider ECG for the following patients:
a) With risk factors:
- Age > 40 years
- History of CAD
- CV risks: DM, HTN, dyslipidemia
- Smoker
b) Unstable vital signs
Imaging – CT, MRI or MRA are indicated if:
- The examination is not consistent with a peripheral lesion.
- Prominent risk factors for CVA are present.
- Neurological signs & symptoms are present.
Nevertheless, there are limitations concerning neuroimaging.
– Non-contrast CT (often used in ED) has low diagnostic yield (2–10%) → a negative CT does not exclude stroke.
– MRI (DWI): Is more sensitive but may still miss 10–22% of strokes within the first 48 hours, especially small posterior fossa infarcts.
– Clinical bedside tests (HINTS, STANDING) can be more reliable than early imaging in detecting central causes of acute vertigo./
Brief overview on the peripheral causes of vertigo
This provides as a concise summary of the peripheral cause of vertigo that I think would be helpful in daily clinical practice. However, do read up more in detail if you have the time.
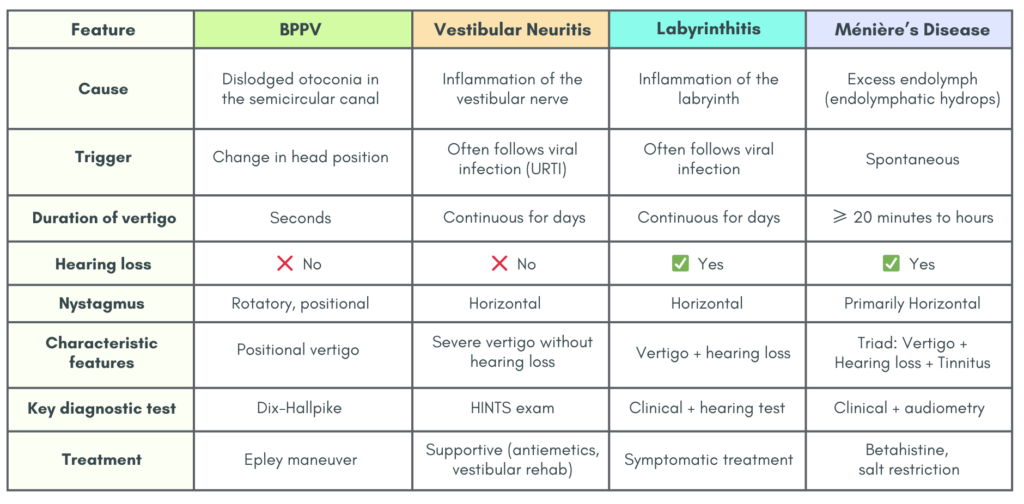
Quick Clinical Clues
- Vertigo lasting seconds + positional trigger –> BPPV
- Vertigo lasting days + no hearing loss –> Vestibular neuritis
- Vertigo lasting days + hearing loss –> Labyrinthitis
- Recurrent vertigo + tinnitus + hearing loss –> Ménière’s disease
Treatment is often tailored to the specific causes of vertigo
Symptomatic treatment may be started for acute vertigo, and these include:
- Anti-emetics: prochlorperazine, metoclopramide
- Antihistamines: promethazine, betahistine
References
- Vanni, S., Vannucchi, P., Pecci, R., Pepe, G., Paciaroni, M., Pavellini, A., Ronchetti, M., Pelagatti, L., Bartolucci, M., Konze, A., Castellucci, A., Manfrin, M., Fabbri, A., de Iaco, F., Casani, A. P., & Società Italiana di Medicina d’Emergenza Urgenza [SIMEU], Società Italiana di Vestibologia [VIS] (2024). Consensus paper on the management of acute isolated vertigo in the emergency department. Internal and emergency medicine, 19(5), 1181–1202. https://doi.org/10.1007/s11739-024-03664-x
- Dommaraju, S., & Perera, E. (2016). An approach to vertigo in general practice. Australian family physician, 45(4), 190–194.
- Vanni, S., Pecci, R., Casati, C., Moroni, F., Risso, M., Ottaviani, M., Nazerian, P., Grifoni, S., & Vannucchi, P. (2014). STANDING, a four-step bedside algorithm for differential diagnosis of acute vertigo in the Emergency Department. Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale, 34(6), 419–426.