Tension Type Headache
Tension Type Headache (TTH)
General features
The female : male ratio is 5:4 where women are only slightly more affected than men.
Average age of onset: 25 – 30 years, peaks between 30 – 39 years, & decreases slightly with age.
Common triggers:
- Stress – mental or physical
- Irregular or inappropriate meals
- High intake or withdrawal of coffee & other caffeine containing drinks
- Dehydration
- Sleep disorders
- Psycho-behavioral problem
- Reduced exercise
- Variations during the female menstrual cycle & hormonal substitution
Proposed pathophysiology
- Activation of hyperexcitable peripheral afferent neurons from head & neck muscles.
- Muscle tenderness & psychological tension
- Abnormalities in central pain processing & generalized increased pain sensitivity
- Genetic factors
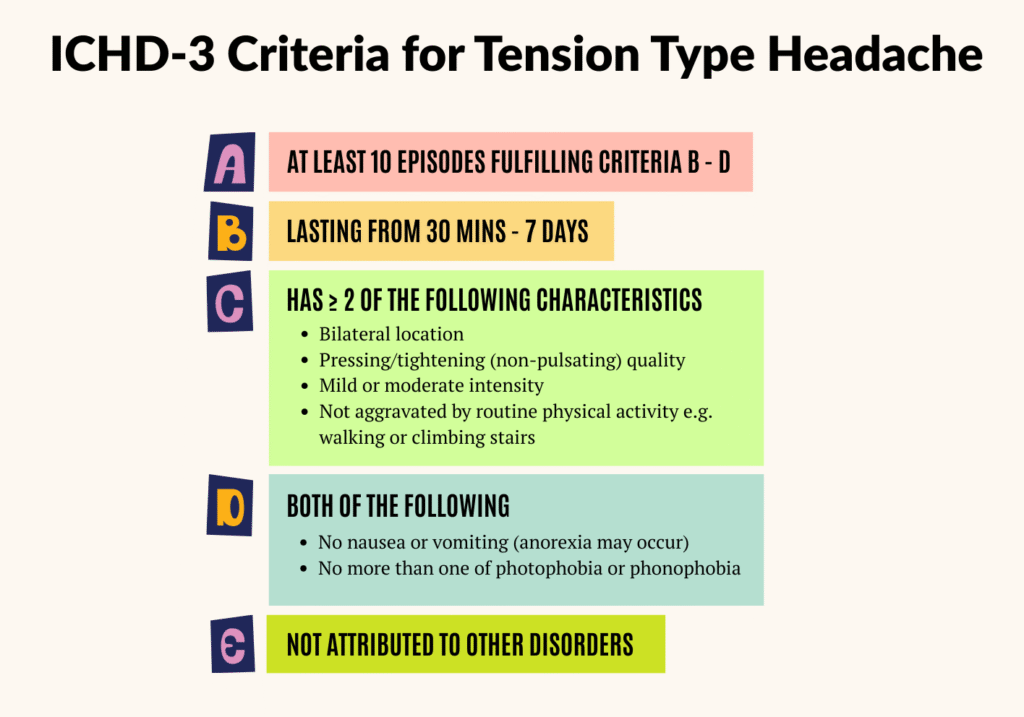
Diagnosis
Tension type headache (TTH) can be diagnosed using The International Classification of Headache Disorders (ICHD-3) criteria as follow:
TTH can be further categorized into subtypes – Episodic (infrequent, frequent) & Chronic
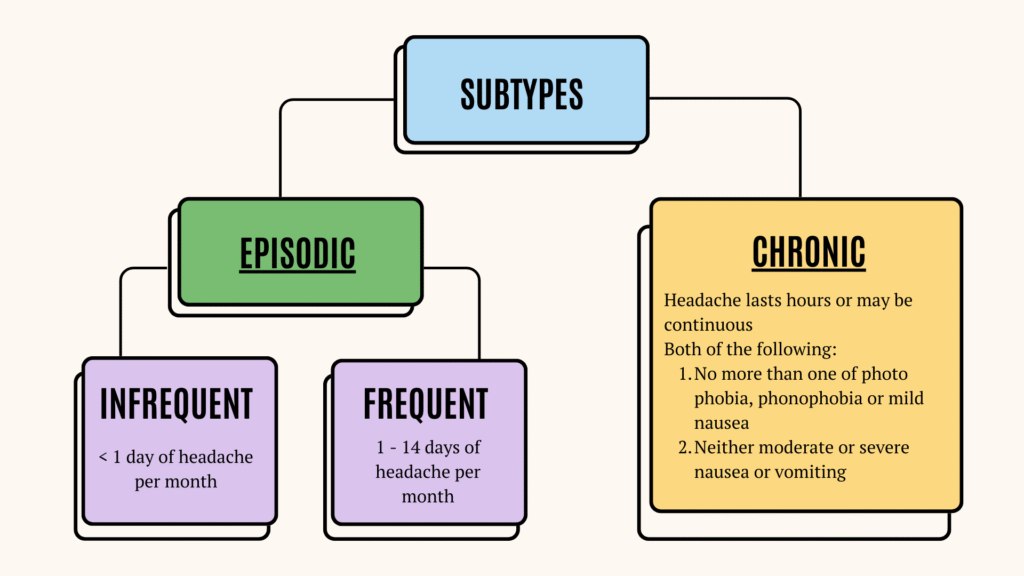
Peripheral mechanisms are probably more important in episodic TTH, whereas central pain mechanisms are pivotal in chronic TTH.
Clinical features of TTH
1. Bilateral
2. Non throbbing (pressing/tightening)
3. Absence of :
- Nausea/vomiting
- Photophobia, phonophobia and osmophobia
- Movement exacerbation.
4. Pericranial tenderness – if present, is the most pronounced & abnormal finding in TTH
- Can be detected by manual palpation.
- Local tenderness may be determined by using small rotating movement with the 2nd and 3rd fingers over the frontal, temporal, masseter, pterygoid, sternocleidomastoid, splenius & trapezius muscles.
Possible co-morbid conditions with TTH
- Sleep apnea
- TMJ disorders
- Fibromyalgia
- Anxiety & depression
- Back pain
- Neck pain
- Irritable bowel syndrome
Management
Consist of pharmacological & non-pharmacological treatment
Pharmacological treatment
Can be divided into:
- Acute therapy – for infrequent or low-frequency episodic TTH
- Prophylactic therapy – for chronic or high-frequency episodic TTH
Both acute & prophylactic therapy can be used together
Acute therapy
Preferred 1st choice – simple analgesics e.g.
- Paracetamol (PCM)
- NSAIDs – Aspirin, Ibuprofen, Ketoprofen, Naproxen, Diclofenac
(There are no clinical trials to support the use of COX-2 inhibitors)
2nd choice – combination analgesics containing caffeine
- More effective than simple analgesics or NSAIDs alone, but more likely to induce medication overuse headache.
Not recommended/No role: Triptans, Muscle relaxants, Opioids
In general, medication for acute treatment should be used not more than 2 – 3 days/week, to minimize chance of overuse or “rebound” headache.
Prophylactic therapy
Indication: For chronic TTH or very frequent episodic TTH.
🥇First line – Amitriptyline (Tricyclic Antidepressant)
- Mechanism: Pain-modulating effect independent of antidepressant action.
- Dose:
– Start low: 10 – 25 mg/day
– Titrate: increase by 10 – 25 mg weekly
– Maintenance: usually 30 – 75 mg/day, better taken 1 – 2 hours before bedtime to avoid the sedative adverse effects. - Common side effects: Dry mouth, drowsiness, dizziness, constipation, weight gain.
- Evaluation: If no response after 4 weeks on maintenance dose, consider switching therapy
🥈Second line
|
Drug |
Dose |
Common side effects |
|
Mirtazapine |
30 mg/day |
Drowsiness, weight gain |
|
Venlafaxine |
150mg/day |
Nausea, vomiting, dizziness, reduced libido |
Treatment notes
- Efficacy of preventive therapy is modest; benefits must outweigh side effects.
- Continue successful therapy for ~6 months, then taper while monitoring headache frequency.
- Resume treatment if headaches recur.
- Avoid medication overuse to prevent chronic daily headache.
Non-pharmacological treatment
General recommendation: Non-pharmacological approaches should be considered for all TTH patients, even though scientific evidence supporting their efficacy is limited.
These include:
1. Education & Lifestyle Changes
- Patient counseling – provide information, reassurance and help identifying headache triggers
- Routine optimization – Encourage regular sleep, exercise and meal schedule
2. Pyscho-Behavioral Therapies
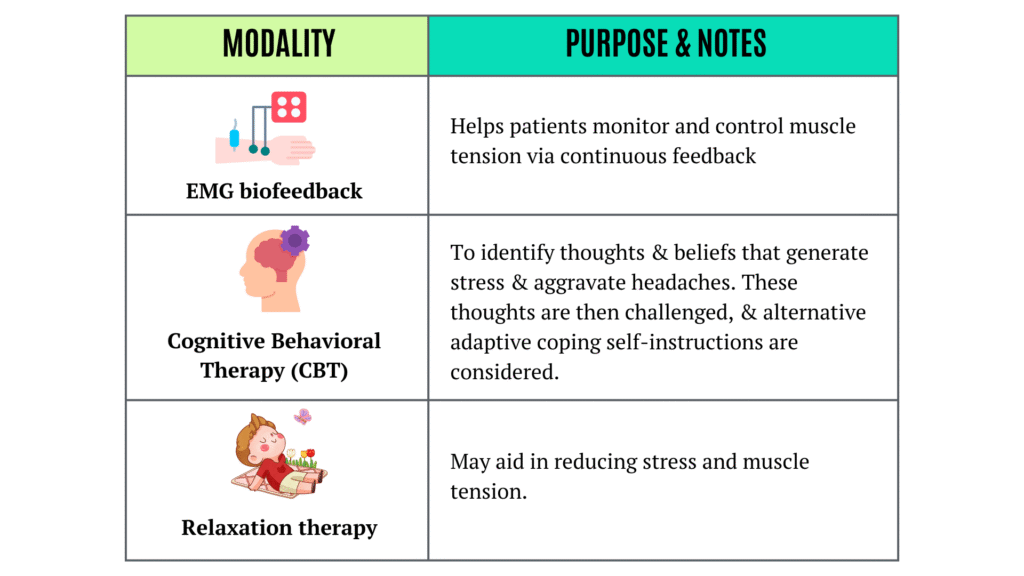
Tailored use:
- CBT – Best for patients with psychological or emotional contributors.
- Biofeedback/relaxation – Preferable for patients with high physical tension.
3. Physical modalities
- Physical therapy and Acupuncture may be helpful, though robust evidence is lacking.
When to refer?
- When the headache diagnosis is unclear
- Patient not responding to treatment
- Headache complicated by medication overuse
- Presence of red flags (SNOOP mnemonic)
Reference
- Bendtsen, L., Evers, S., Linde, M., Mitsikostas, D.D., Sandrini, G. and Schoenen, J. (2010), EFNS guideline on the treatment of tension-type headache – Report of an EFNS task force. European Journal of Neurology, 17: 1318-1325. https://doi.org/10.1111/j.1468-1331.2010.03070.x
- Loder, E., & Rizzoli, P. (2008). Tension-type headache. BMJ (Clinical research ed.), 336(7635), 88–92. https://doi.org/10.1136/bmj.39412.705868.AD
- Merican, J. S., Goh, K. J., Wan Sulaiman, W. A., Chan, P. H., Puvanarajah, S. D., Tai, M. L., & Chee, K. Y. (2021). Consensus guidelines on the management of headache 2021 [PDF]. Malaysian Society of Neurosciences.