Dementia
Dementia
(Focusing on Primary Care)
Dementia is a chronic, progressive neurodegenerative disorder characterized by a decline in cognitive function (i.e. ability to process thought) deteriorates progressively.
It affects memory, thinking, orientation, calculation, learning capacity, language, judgement, emotional control, social behavior, or motivation.
The term Dementia is now called Major Neurocognitive Disorder (MND) as per DSM-5
Either the DSM-5 or ICD-10 criteria can be used for the diagnosis of dementia.
In this post, we will discuss mainly based on DSM-5 criteria.
DSM-5 criteria
To diagnose MND, there must be:
- Significant decline in at least one of the following neurocognitive domains:
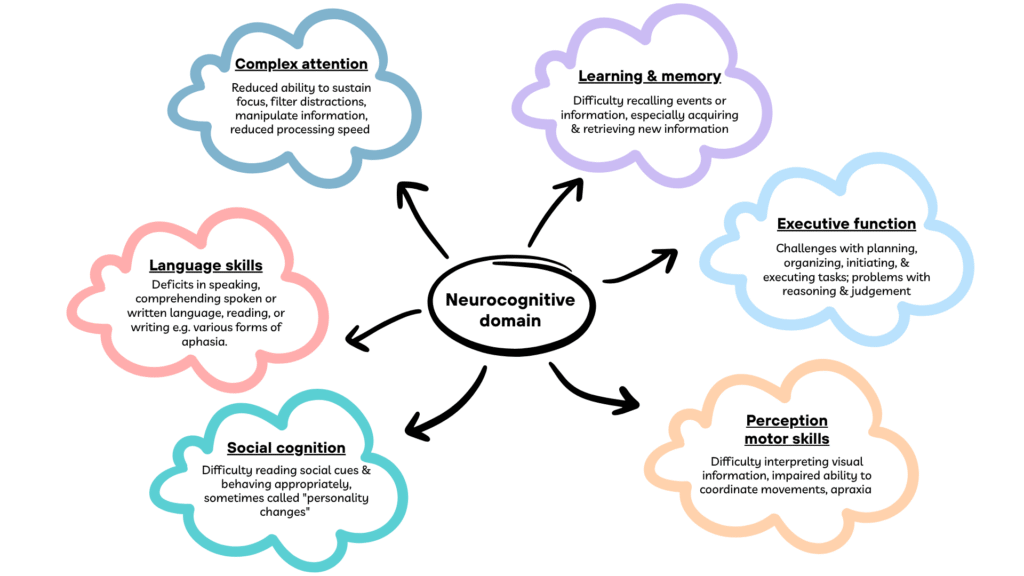
- These decline may be discovered by either the individual him-/her-self, a knowledgeable informant or the clinician.
- A substantial impairment in cognitive performance, preferably documented by standardized neuropsychological testing or in its absence, another quantified clinical assessment.
- The cognitive deficits interfere with independence in everyday activities.
- The cognitive deficits do not occur exclusively in the context of delirium.
- The cognitive deficits are not better explained by another mental disorder (e.g. MDD, schizophrenia)
The DSM-5 further delineate 13 subtypes of MND including:
- Alzheimer’s disease
- Vascular disease
- Lewy body disease
- Frontotemporal degeneration
- Traumatic brain injury
- Substance/medication use
- HIV infection
- Prion disease
- Parkinson’s disease
- Huntington’s disease
- Another medical condition (e.g. progressive supranuclear palsy,
corticobasal syndrome, & less commonly, multiple system atrophy) - Multiple etiologies
- Unspecified
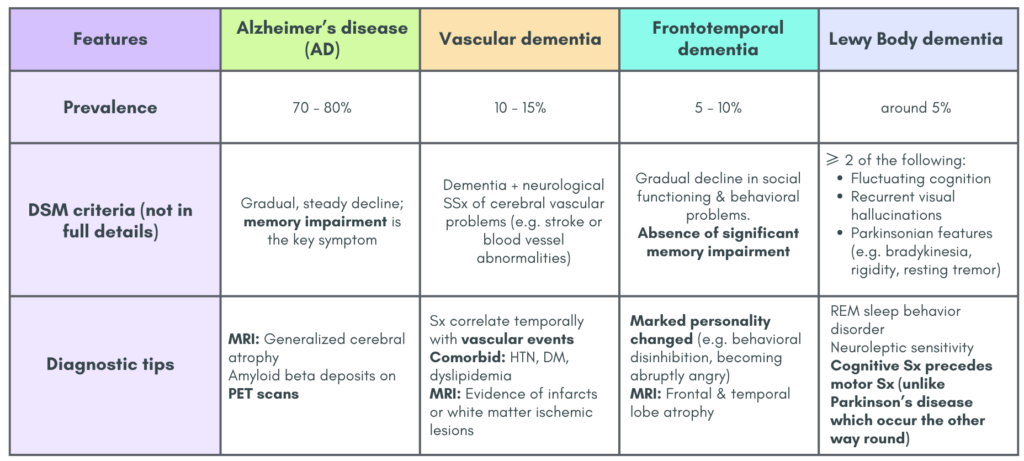
Features of some of the dementia types
Additional notes
- Mixed dementia is a combination of 2 or more dementia types, where AD + vascular pathology is the most common.
- In early-onset AD (< 65 years old), patient may present with behavioral (frontal), visual (posterior cortical atrophy) or language (logopenic) variants with relatively well-preserved memory until the later stages of the disease.
Risk factors
Non-modifiable
- Advancing age (≥ 65 years)
- Gender: Female
- Genetic
Modifiable
- CV risk factors: HTN, DM, hyperlipidemia, obesity & smoking –> Vascular dementia
- Psychiatric illness e.g. depression
- Lifestyle: smoking, excessive alcohol consumption, physical inactivity, social relationship
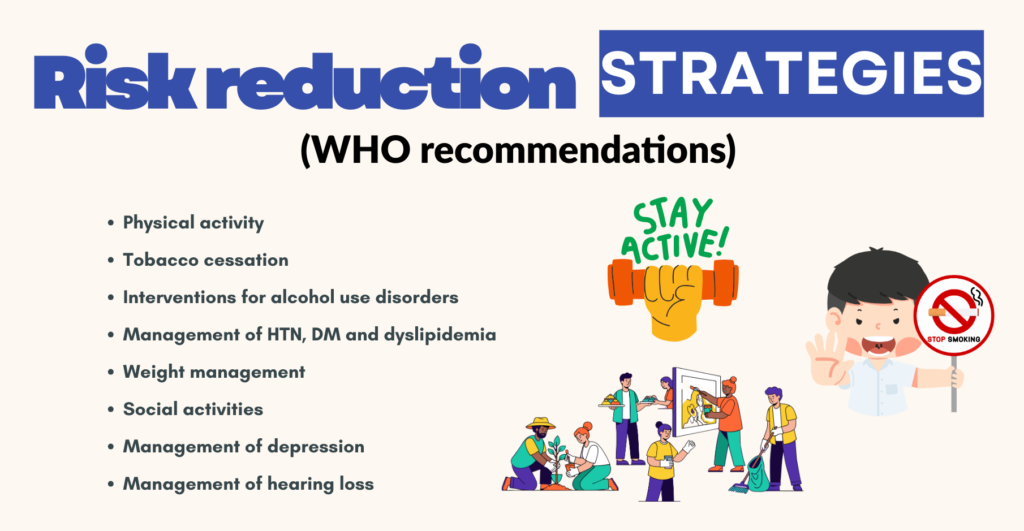
There is insufficient evidence to support the use of medication (e.g. aspirin & statins), vitamins and supplements to prevent dementia.
History taking
Should include
1. Cognitive assessment (according to the neurocognitive domain as listed in the DSM-5)
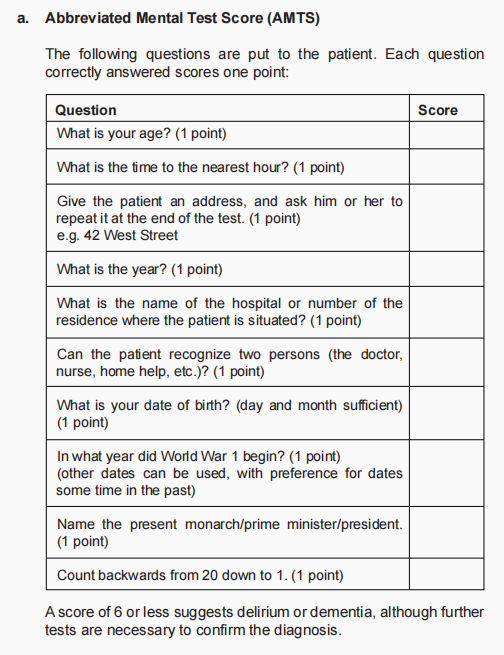
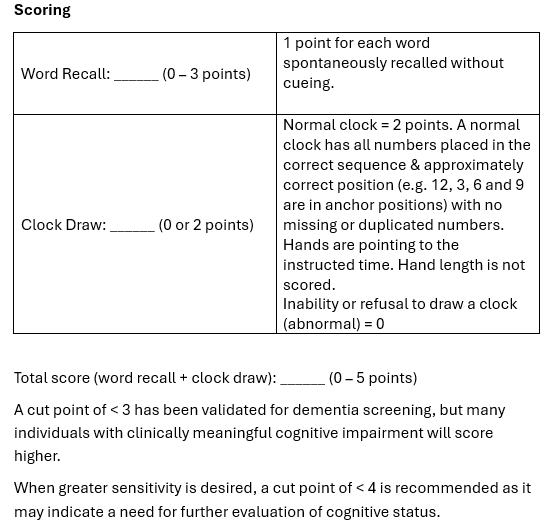
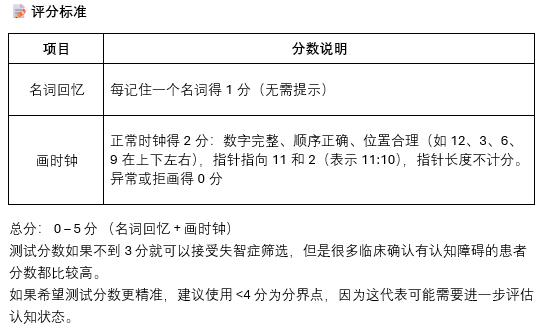
- Assessment tools that may be more practical in primary care: Mini-Cog, Abbreviated Mental Test Score (AMTS), Mini-mental status examination (MMSE)
- Diagnostic consideration:
– Should not based on cognitive assessment score solely.
– Functional decline in daily tasks should also be present to meet diagnostic criteria - Role of cognitive scores: To support diagnosis & to monitor disease progression
2. Non-cognitive assessment: Functional status (ADL), Behaviors, Emotion, Caregiver burden
3. Severity of dementia according to functional status
- Mild: Difficulties with instrumental activities of daily living (e.g. housework, managing money)
- Moderate: Difficulties with basic activities of daily living (e.g. feeding, dressing)
- Severe: Fully dependent
4. CV risk factors
5. Current drugs/medications
Cognitive assessment tools
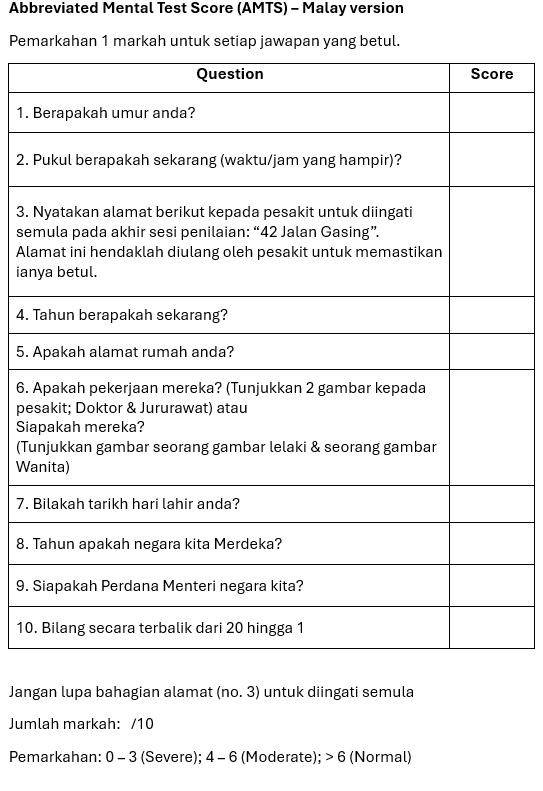
Abbreviated Mental Test Score (AMTS)
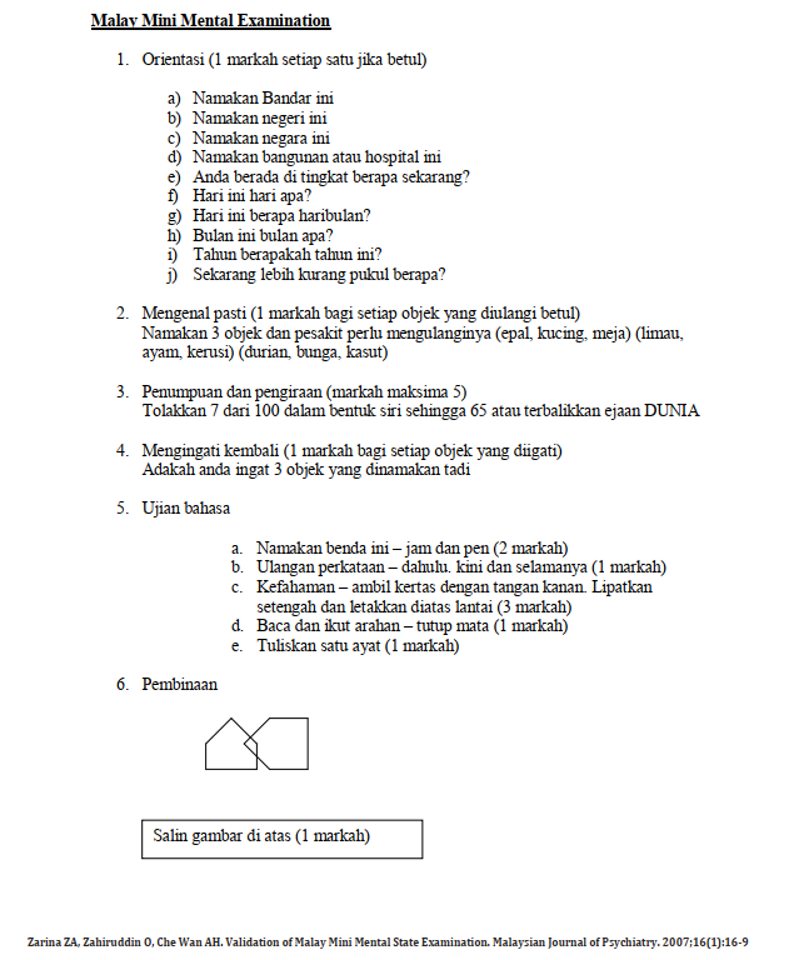
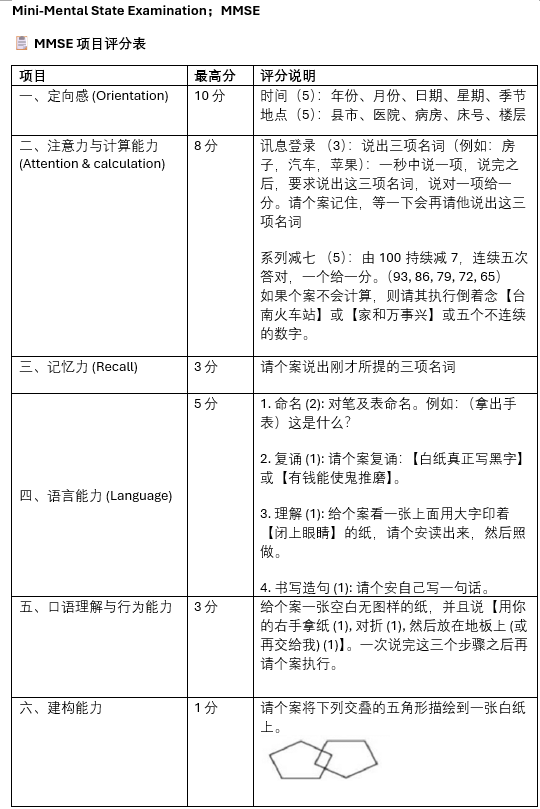
Mini Mental Score Examination (MMSE)
MMSE Score interpretation:
24 – 30: Normal cognitive function
18 – 23: Mild cognitive impairment
0 – 17: Severe cognitive impairment
Factors that can affect performance:
- Physical/neurological problems
- Educational level
- Language/speech problem
- Intellectual disability
The Chinese version of the MMSE actually included score interpretation according to educational level:
a) Secondary school and above
< 24: Mild cognitive impairment
< 16: Severe cognitive impairment
b) Primary school: < 21 – abnormal
c) Uneducated: < 16 – abnormal
Source: orgws.kcg.gov.tw/001/KcgOrgUploadFiles/117/relfile/0/73016/d45b03ce-9569-4484-b51d-09e45ef02fd2.pdf
Mini-Cog
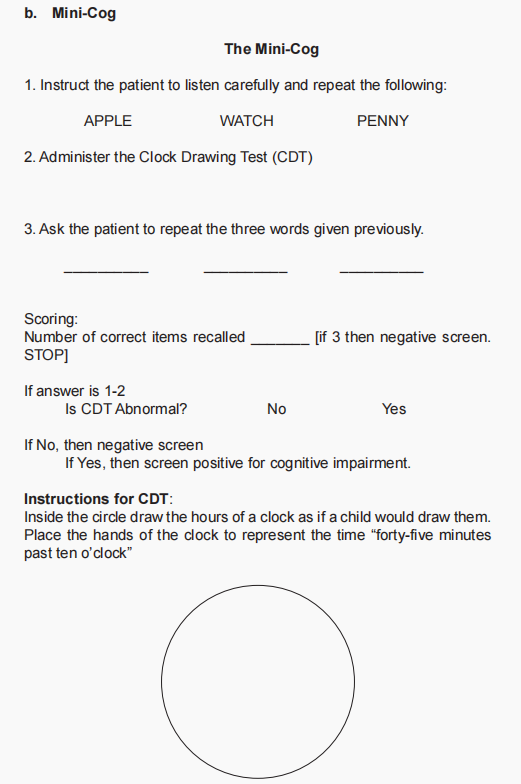
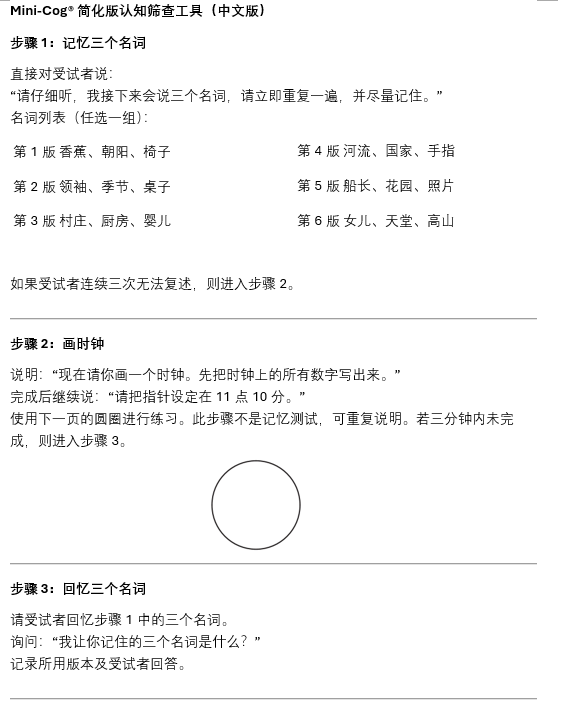
Among these three assessment tools, only the MMSE has been validated in local languages – Malay, Mandarin.
Physical examination
Should include:
- Vision 👀
- Hearing 👂
- Focal neurological factors 🧠
- Involuntary movements
- CV risk factors 🧡
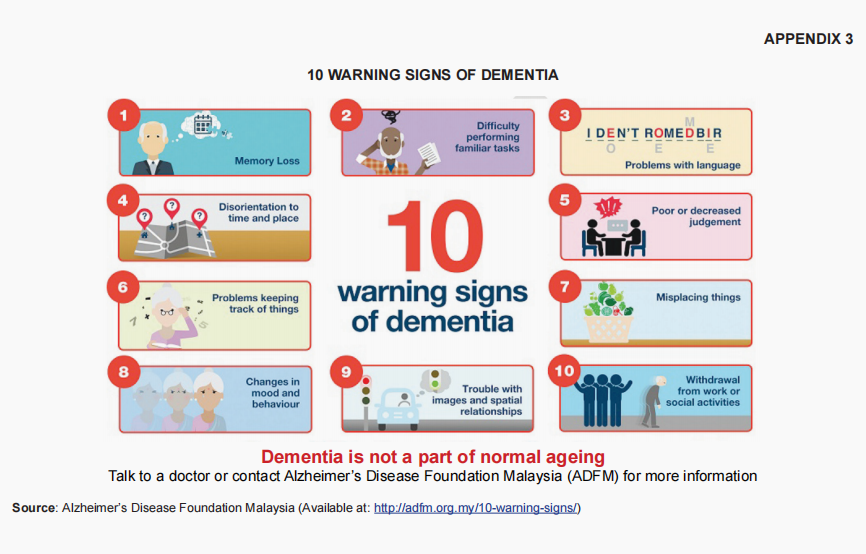
Warning signs 🚨
Dementia mimicking conditions
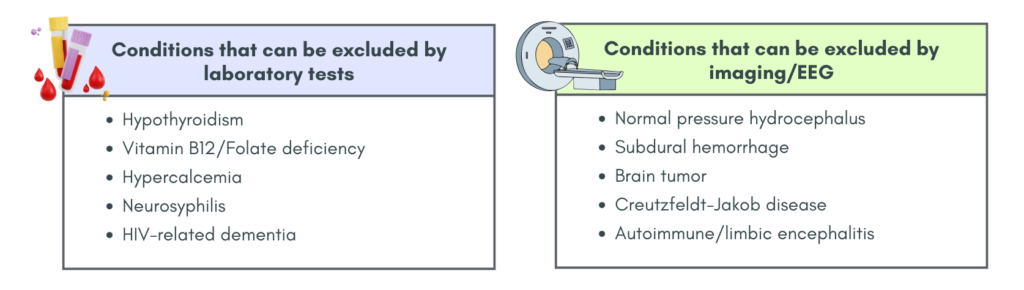
Investigations
Mainly TRO dementia mimicking conditions as above.
These investigations may include:
- FBC, RP, LFT
- Calcium, B12, Folate
- TFT
- VDRL & anti-HIV if indicated.
- Brain imaging
– Structural neuroimaging (CT or MRI) – TRO reversible causes & other intracranial pathology
– Functional neuroimaging – Not routinely done, but may be considered if the diagnosis of dementia is uncertain - EEG should be considered in rapidly progressive cognitive decline & atypical features of dementia.
– A normal EEG result render a diagnosis of Lewy Body Dementia very unlikely. - CSF biomarkers
– Lumbar puncture may be considered to examine the CSF for amyloid and phosphorylated tau proteins.
– However there are insufficient evidence to support its routine use.
Non-pharmacological management (individualized)
1. Mainstay
- Involvement of caregiver
- Communication skills
- Person centered care
- Activity for engagement – ADL, hobbies, social engagement
Caregivers
Should be involved from the beginning (integral part of management)
Training (professional & non-professional) [NICE recommendation] may include:
- Education about dementia on its symptomatology & natural progression
- Development of personalized strategies & carer skills
- Training on care of person with dementia, including understanding & responding to changes In behavior.
- Training in communication skills
- Advice on carers’ own physical, mental health & spiritual wellbeing. (the Zarit Caregiver Burden Assessment [ZBI] can be used to assess the burden of caregivers)
- Information on relevant services & their access
- Advice on planning for the future.
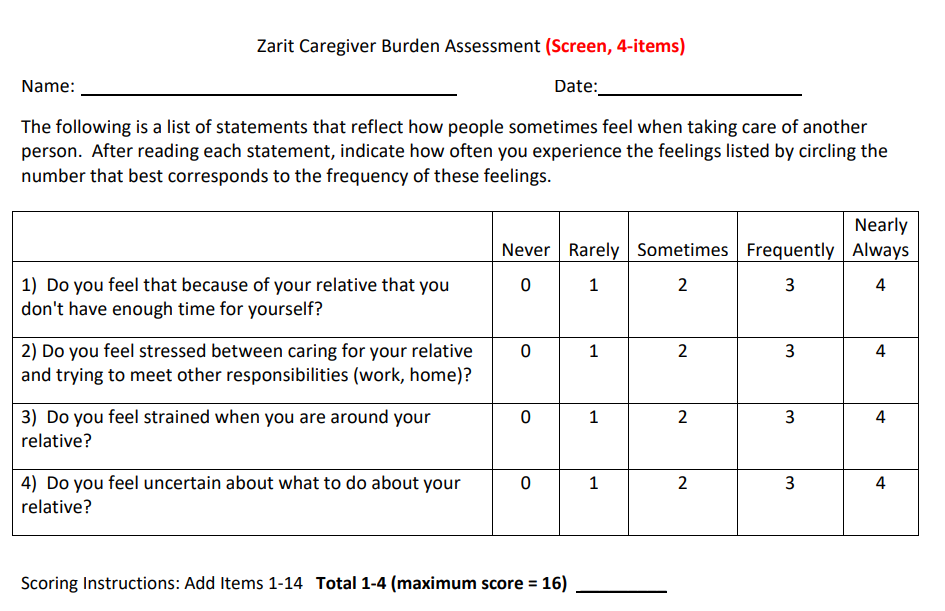
The 4-items ZBI assessment can be used as a screening, which may be more useful in primary care.
There are also a more detailed assessment which comprised of 12-items and 22-items.
2. Structured non-pharmacotherapy
- Cognitive stimulation therapy by occupational therapist to enhance cognition & engagement, recommended in people with mild to moderate dementia.
- Cognitive rehabilitation or occupational therapy to support functional ability.
3. To manage the behavioral and psychological symptoms if present, by:
- Exploring & addressing possible clinical or environmental cause/triggering factors.
- Offer psychosocial & environmental interventions as initial & ongoing treatment:
– Psychological intervention (e.g. CBT) for depressive symptoms &/or anxiety.
– Personalized & tailored activities for agitation & aggression.
3. Others
- Music therapy, art therapy, aromatherapy, massage, mindfulness, pet therapy… etc. Nevertheless, most of these are based on low to moderate quality of evidence.
Pharmacological treatment 💊
Mainly:
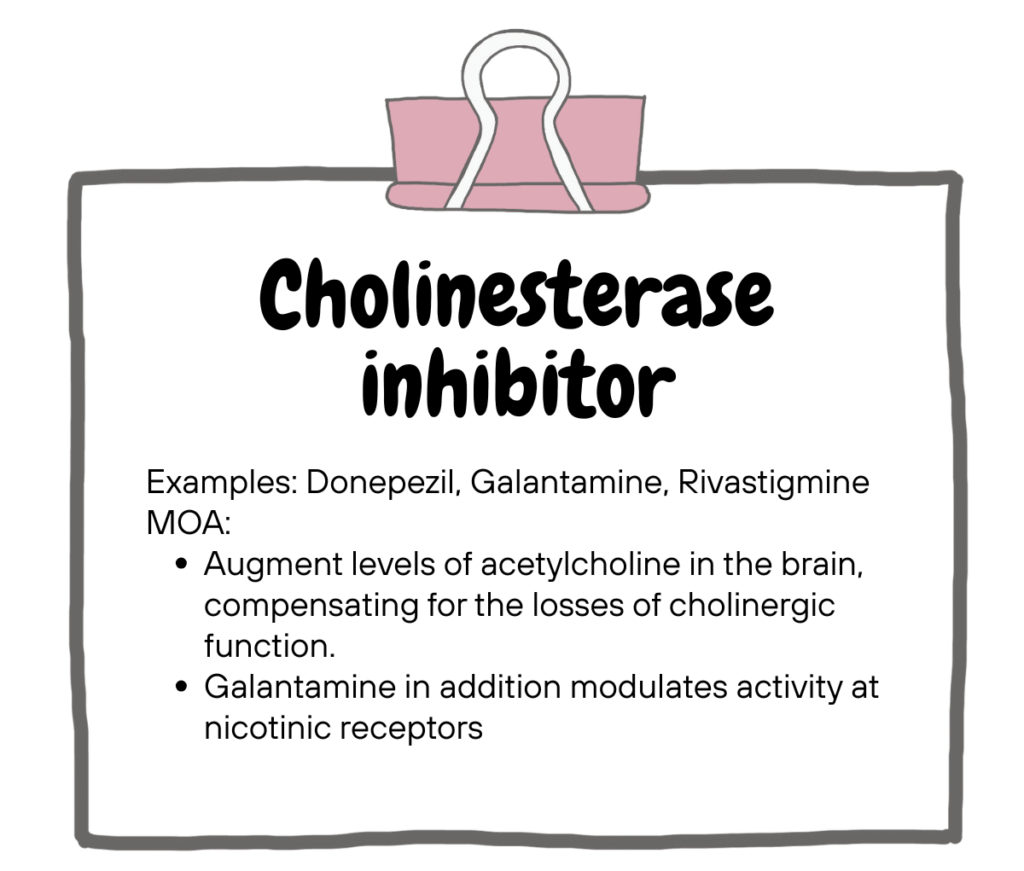
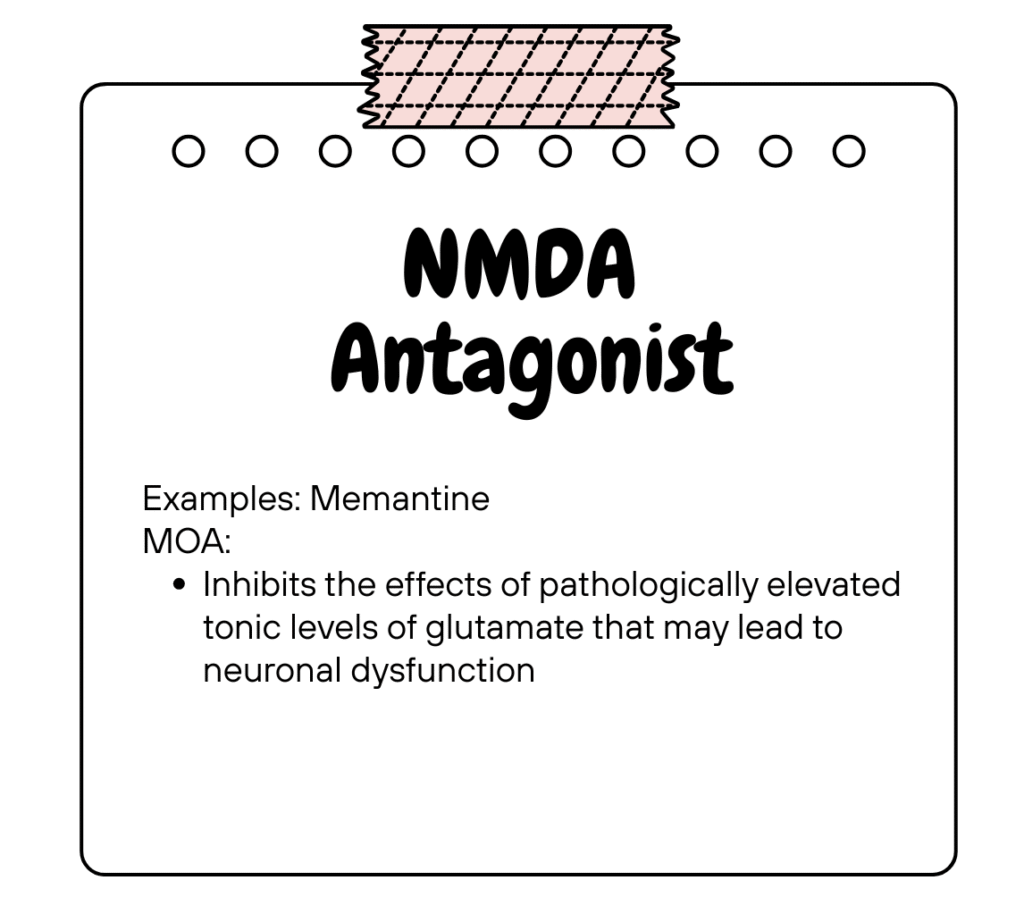
Keep in mind that these pharmacological treatment are not curative, but rather aimed at managing symptoms (cognitive, non-cognitive & behavioural), improve independence & preserve function.
Under the MOH Medicines Formulary, donepezil, rivastigmine & memantine are listed & indicated for the use in AD while only rivastigmine is indicated for PDD.
Regarding medication for behavioural & psychological symptoms
Antipsychotics (AP) may be considered if they have a risk of harming themselves or others.
- US FDA issued a warning regarding increased mortality associated with the use of AP in elderly patients with dementia-related psychosis.
- If starting on AP, NICE recommends the lowest effective dose for the shortest possible duration & patient should be reassessed regularly. AP should be wean off if it is not needed.
Antidepressants:
- May be considered for those who have agitation.
- May be prescribed for those with pre-existing severe mental health problem.
No role for mood stabilisers to treat agitation.
While some studies suggest modest benefits of Ginkgo biloba (EGb761) for cognitive decline, particularly in mild cognitive impairment and early-stage dementia, the evidence is inconsistent due to heterogeneity in study designs and patient populations. Overall, the results indicate small improvements, but further high-quality trials are needed to confirm its efficacy and safety.
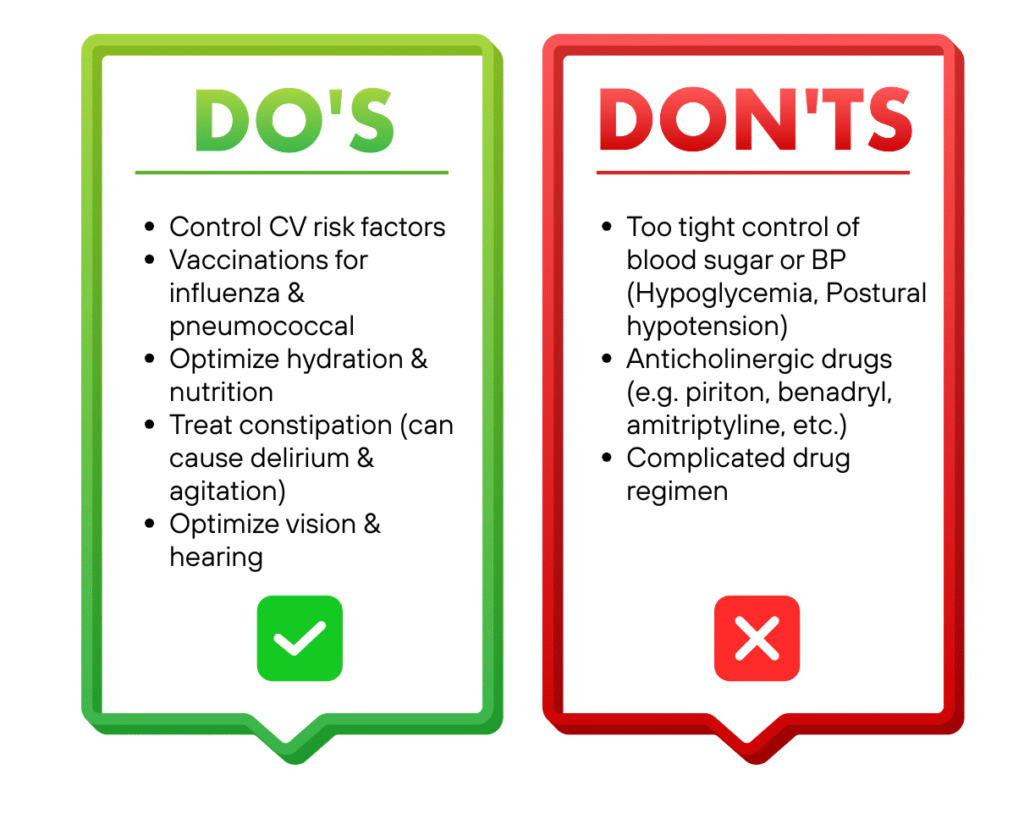
Some DOs and DON’Ts
Other aspects of management
Driving assessment 🚗
- Driving ability involves multiple cognitive domains & requires visuospatial, executive function, memory, attention & motor skills.
- Assessment of fitness to drive involves composite cognitive test batteries in combination with other types of assessment e.g. driving simulator test or on-road test.
- Driving risk may be greater in certain subtypes of dementia e.g. FTD (due to lack of cortical insight) & DLB (due to fluctuating consciousness & visual hallucinations)
- Refer occupational therapist for driving assessment, especially for moderate/severe dementia.
Legal aspect/ethical issues
- If there’s doubt about a person with dementia’s (PWD) decision-making capacity, a formal assessment should be done. If they lack capacity, a surrogate decision-maker must act in their best interest.
- PWD can make advance decisions about treatment while they have capacity, through an advance directive or care plan, which the healthcare practitioner should honor if it was made when the patient had capacity.
Referral 📝
All patients suspected of dementia should be referred to a specialist (e.g. geriatrics/psychiatry/neurology) for confirmation of diagnosis due to the need for comprehensive assessments & investigations.
The medication for dementia are also not available in primary care setting.
Once a diagnosis is made, stable PWD can be co-managed in both primary & secondary/tertiary care as an integrated care system.
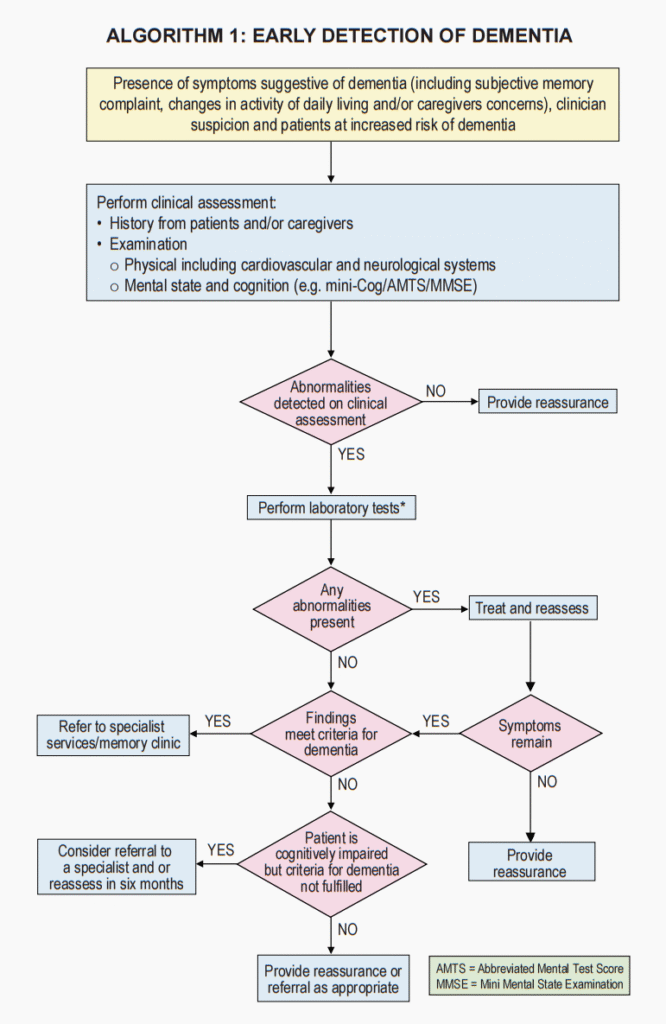
Algorithm
Other considerations
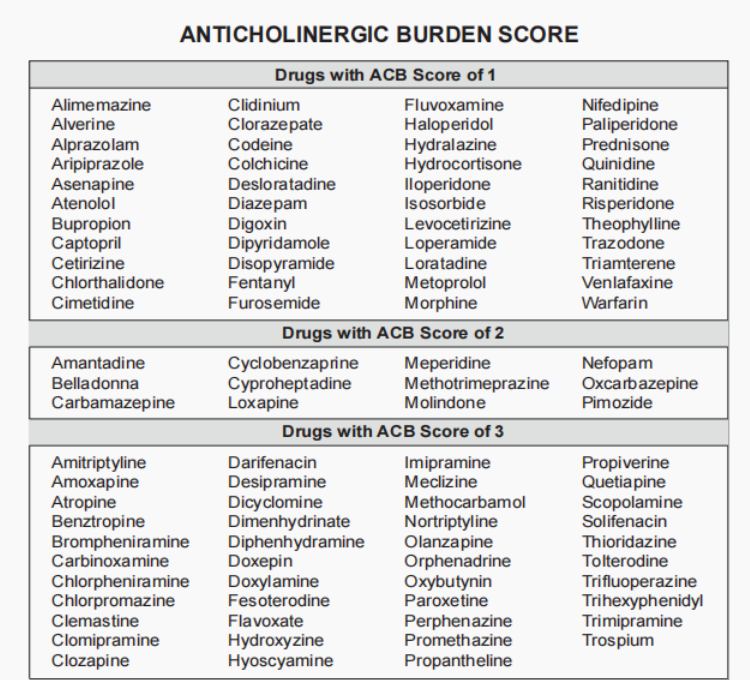
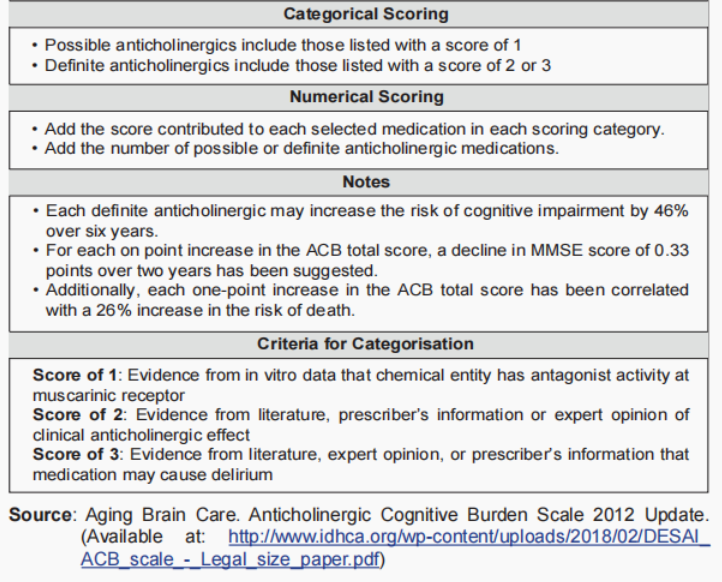
In patient with cognitive impairment, we should be cautious in prescribing medications with anticholinergic properties to avoid worsening of their symptoms.
Below are medications with their anticholinergic burden score as listed in our Malaysia CPG guideline.
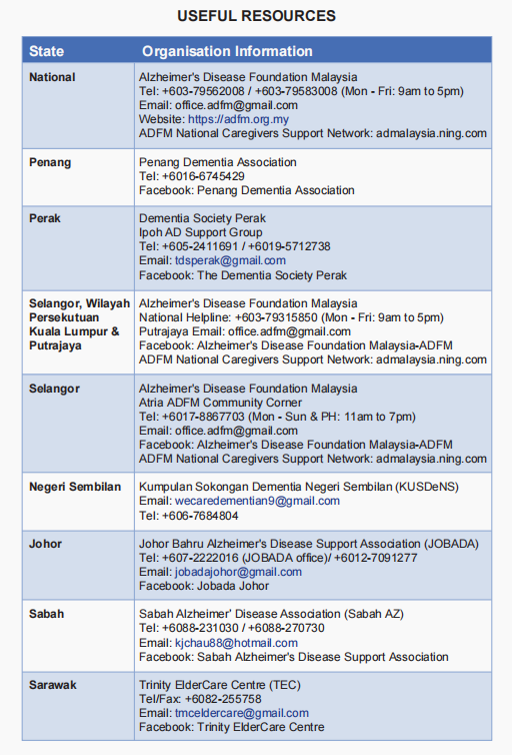
Useful resources for caregiver
References
- Ministry of Health Malaysia. 2021. Clinical Practice Guidelines: Management of Dementia, Third Edition.
- Emmady PD, Schoo C, Tadi P. Major Neurocognitive Disorder (Dementia) [Updated 2022 Nov 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557444/
- Major Neurocognitive Disorder (MND): DSM-5 Differential Diagnosis. https://www.thecarlatreport.com/ext/resources/factsheets/factsheetlibrary/Major-Neurocognitive-Disorder-Differential-diagnosis.docx.pdf?1699028917