Approach to tremors
Approach to Tremors
Definition: Tremor is defined as an involuntary, oscillatory & rhythmic movements of a body.
It is quite commonly seen in primary care settings either as a main complaint or as an incidental finding.
This post is mainly on discussing regarding the approach to tremors, though not too in-depth but hopefully relevant and practical in our daily practices.
Approach
A consensus statement by Bhatia et al. has proposed the classification of tremors along two axes:
- Axis 1 – clinical characteristics, including historical features (age of onset, family history & temporal evolution), tremor characteristics (body distribution, activation condition), associated signs (systemic, neurological), and laboratory tests (electrophysiology, imaging)
- Axis 2 – etiology (acquired, genetic or idiopathic)
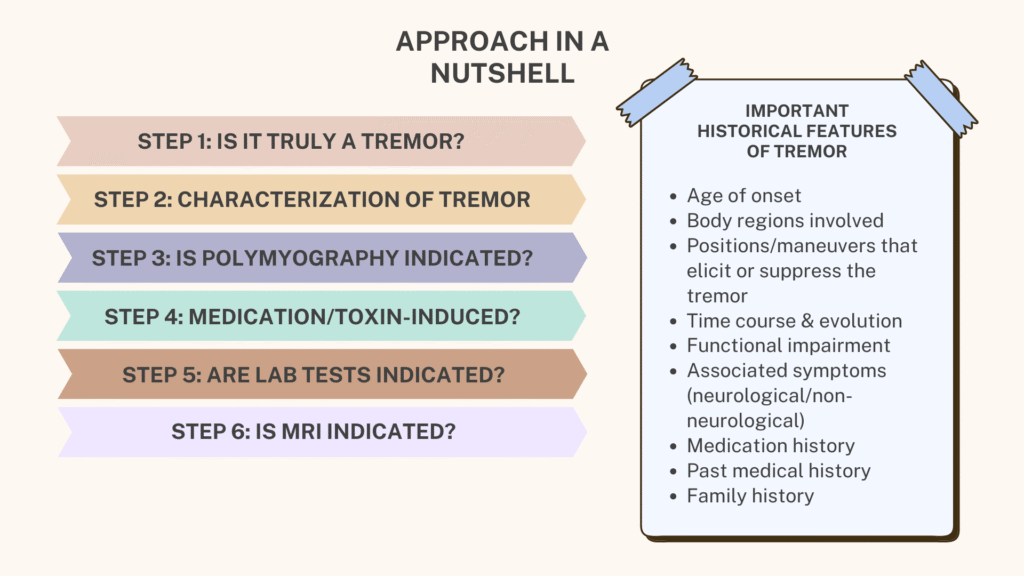
The consensus statement has listed 8 steps to help classify tremors based on these 2 axes.
Step 1: Is the movement disorder really tremor? (Is it truly a tremor)
Tremor needs to be differentiated from other hyperkinetic movement disorders, especially myoclonus, as well as tics and chorea.
Myoclonus is generally a sudden, fast, brief & jerky unidirectional movement, in contrast to tremor which is oscillatory & rhythmic.
- Diagnostic aid: Polymyography helps distinguish myoclonus from tremor.
- Note: myoclonus & tremor may coexist.
Once it is ascertained that the movement disorder is truly a tremor, next step is to characterize the tremor.
Step 2: Characterization of tremor
Tremors may be characterized based on its activation pattern, topographical distribution and frequency. Of these, characterization based on activation pattern, supplemented by topographical distribution is a practical approach in clinical settings.
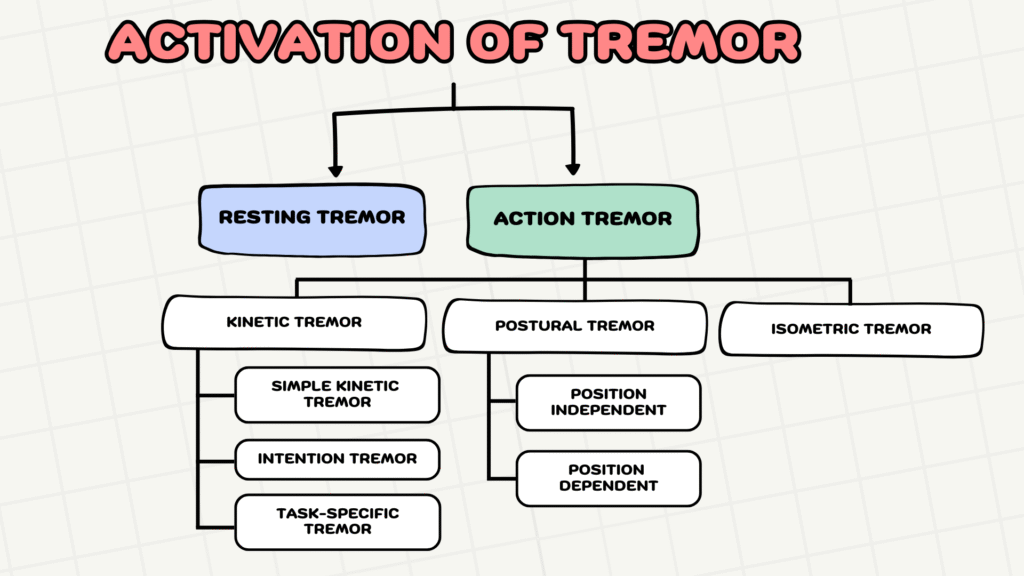
The activation pattern of tremor can be either:
- Resting OR
- Action, subdivided into kinetic, postural and isometric
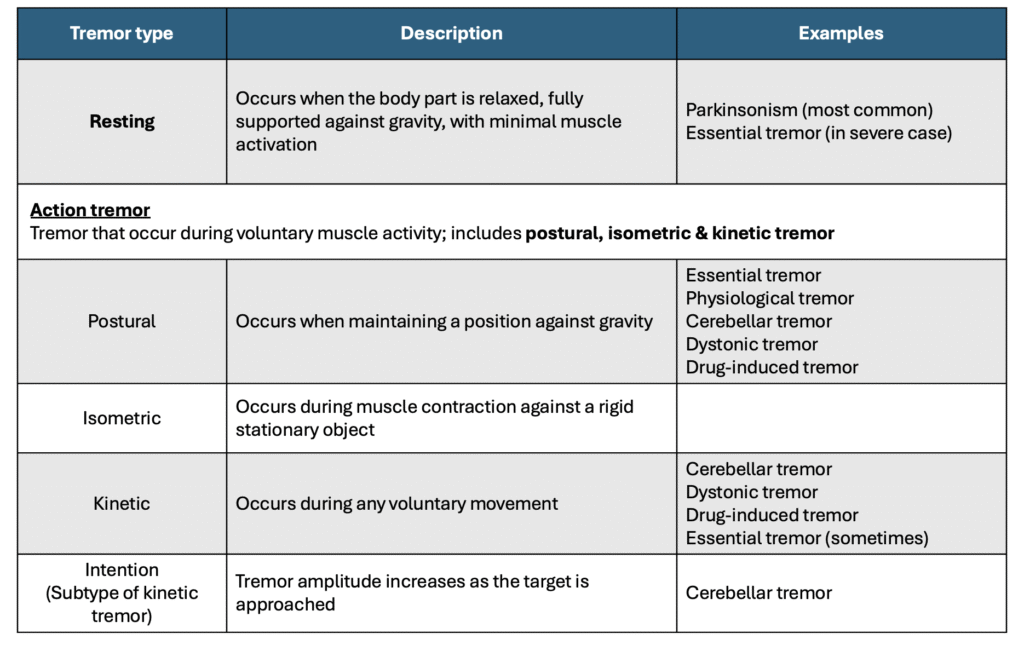
Further description & examples of tremor based on their activation pattern
Assessing for resting tremor

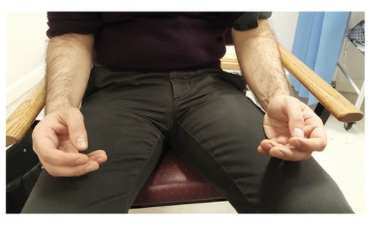
i. Ask the patient to rest his/her arm on the armchair, with forearm supported & the hands hanging freely over the arm rest – Figure (a) or
ii. Position the patient with both forearms resting on the thighs in a semi‑pronated, relaxed position – Figure (b). Supination should be avoided, as it activates the biceps muscle and therefore may not represent a true resting tremor.
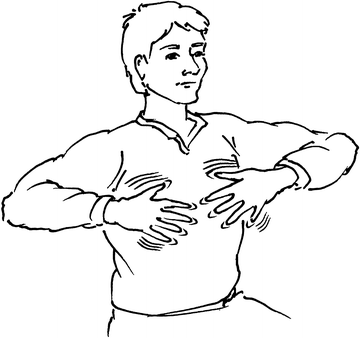
Cognitive & Motor Co-activation
When resting tremor is subtle, cognitive or motor co‑activation can be used, with the patient performing a task while the examiner evaluates tremor amplitude.
These tasks can be:
- Cognitive tasks – Ask patient to count backwards from 100, perform serial sevens, or spell a difficult word.
- Motor tasks – Ask the patient to perform tapping movements with the opposite hand.
When performing these cognitive/motor tasks, observe for the tremor amplitude.
- In Parkinson’s tremor: Tremor amplitude increases
- In function (psychogenic) tremor: Tremor amplitude reduces
Another important concept to know is regarding re-emergent tremor.
Re-emergent tremor is when there is transient suppression (1 – 2s) of tremor amplitude during voluntary movement, after which the tremor return to its normal amplitude. This is often seen in Parkinson’s tremor.
Assessing for action tremor
A. Postural tremor

Ask the patient to extend the arms in prone position & observe for any tremor in this position.
Assess also tremor in varying positions, as position‑dependent tremor—appearing only in specific position—suggests dystonic tremor
Lastly, assess for any tremor in the wing-beating position as below
Wing-beating tremor is classically seen in Wilson’s disease, but it may also be seen in Holmes tremor.
B. Kinetic tremor
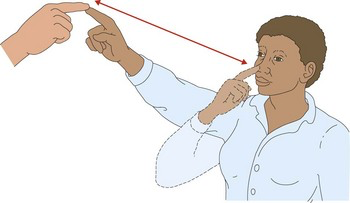
i. Ask patient to perform slow finger-to-nose testing:
- Constant tremor amplitude –> simple kinetic tremor
- Increasing amplitude near target –> intention tremor
ii. Assess task-specific tremor (e..g writing)
iii. Ask patient to draw spirals with each hand separately, unsupported by the table

Large shaky spiral is suggestive of essential tremor whereas small, quivery spiral points towards Parkinsonism
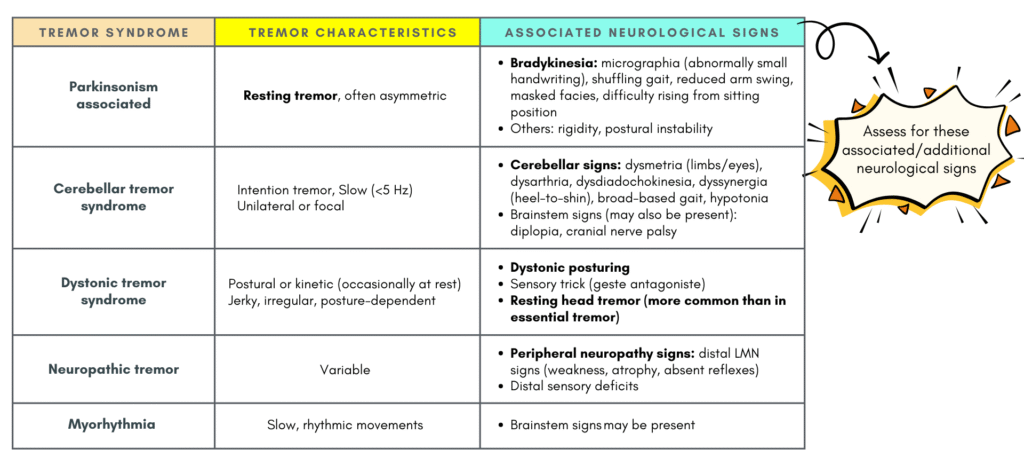
Step 2.1 Assessing for additional neurological signs
After assessing tremor activation, next is to look for any additional neurological signs.
Tremor can occur as either:
- Isolated tremor syndrome (tremor alone) or
- Combined tremor syndrome (tremor + other neurological signs)
The table below shows some of the combined tremor syndrome and their associated neurological signs that we should keep a lookout for.
Step 3: Is polymyography indicated?
Indications for polymyography:
- To make distinction between tremor & myoclonus.
- Objective assessment of signs associated with functional tremor, such as entrainment & distractibility.
- To differentiate between Enhanced Physiological Tremor & Essential Tremor.
- Selecting appropriate muscles for botulinum toxin treatment in patients with dystonic tremor.
Step 4: Is the tremor medication or toxin-induced? 💊
Assess patient’s medication history, especially when they present with new/sudden-onset tremor.
Examples of tremor inducing medications:
- Lithium
- Antipsychotic
- Amiodarone
- Steroids
- Stimulants
- Levothyroxine
- Antidepressants (SSRIs/TCAs)
- Caffeine/Nicotine
Step 5: Are laboratory test indicated? 🔬
Laboratory investigations are usually done to identify acquired cause or treatable metabolic disorders, as tremor may arise from conditions such as renal failure, hepatic failure, hyperthyroidism or altered glucose metabolism.
Recommended basic laboratory tests especially in patients with bilateral isolated tremor syndrome include:
- Thyroid function test
- Liver function test
- Renal profile
- Glucose & electrolytes – to look for hypoglycemia, hypocalcemia, hyponatremia, hypomagnesemia
Other tests as indicated:
- Serum catecholamines – if there are other symptoms of pheochromocytoma e.g. episodes of headache, sweating &/or tachycardia.
- Test for toxins if there is a history of exposure.
- Serum copper, ceruloplasmin – to rule out Wilson disease especially if the tremor is combined with dystonia or a family history of movement disorders & cognitive or psychiatric symptoms.
Step 6: Is an MRI indicated?
MRI may be done if structural cause is suspected.
Proposed indications for MRI, mainly for combined tremor syndrome:
- Focal/unilateral tremor
- Non-classical in appearance
- In cases where there is a sudden onset or stepwise deterioration
- Family history of movement disorders combined with cognitive or psychiatric symptoms
Isolated tremor syndrome usually do not require MRI unless there is suspicion of an acquire cause (sudden onset or stepwise deterioration, unilateral) or a family h/o movement disorders combined with cognitive or psychiatric symptoms.
Step 7 & Step 8
Step 7: Is presynaptic dopamine transporter imaging indicated?
Step 8: Are genetic tests indicated? – Generally genetic testing is only considered in patients with combined tremor syndrome & a relevant family history.
Both of these steps would not be discussed in details here as they are mainly considered at tertiary level.
Note: It is important to evaluate for any functional impairments due to the tremor, as this will decide whether treatment should be initiated or not. This is due to the fact that all current treatments are symptomatic, and non-disease modifying.
Another clinical approach
In addition to the steps as discussed above, there is another approach that is somewhat similar but in a more concise way and perhaps more applicable in primary care settings.
This approach consists of asking 3 ‘cardinal’ questions:
1. Does the tremor require urgent evaluation?
- An abrupt onset & rapid progression (days to weeks) are concerning.
- Rapidly progressive tremor accompanied by neurological signs such as dysarthria, ataxia, seizures, or gait disturbance warrants urgent neurological assessment, as it may reflect an acute toxic etiology (drug-induced e.g., lithium or valproic acid). A thorough medication history, serum drug levels, and consideration for emergency admission should be considered.
2. Is further investigation or treatment required in primary care?
- In patients with isolated upper limb action tremor, blood test e.g. renal function, thyroid function, liver function test, electrolytes TRO reversible causes can be done.
- In young-onset cases (<40), consider excluding Wilson’s disease with LFT, serum ceruloplasmin, & copper.
- In the absences of reversible causes & the presence of functional impairment, consider treating as essential tremor.
3. Does the patient need referral for specialist assessment?
- All cases with clinical syndrome rather than essential tremor (ET) should be referred.
- ET cases refractory to medication. with functional limitations would also benefit from diagnostic evaluation by specialist.
Brief overview of tremors
This section will discuss briefly some of the tremors (just to give an idea) that may be encountered and managed within the primary care settings. A detailed discussion regarding these tremors will be done in another post.
A. Enhanced physiologic tremor
Physiologic tremor is present in all people, but it is usually imperceptible.
Nevertheless, this tremor can be enhanced by anxiety, stress, certain medications & metabolic conditions.
A tremor that comes & goes with anxiety, medication use, caffeine intake, or fatigue usually do not require further testing.
B. Functional tremor
Previously also known as psychogenic tremor.
Characteristics of the tremor:
- Sudden onset
- Variable features – changing characteristics, location & frequency
- Improves with distraction; Entrainment positive
- Spontaneous remission/response to placebo
- No neurological findings or lab abnormalities
- May be linked to psychiatric conditions or sometimes secondary gain
Often there is a stressful life event that precedes the tremor.
C. Essential tremor
The most common pathological tremor.
It is a action tremor, often involving bilateral hands, and sometimes the head, lower limbs & voice.
No additional neurological findings.
Autosomal dominant in ~50% of the cases.
Can manifest during early adulthood, but due to its slow progression, most patients usually present at around 60+ years old for treatment.
References
- van de Wardt, J., van der Stouwe, A. M. M., Dirkx, M., Elting, J. W. J., Post, B., Tijssen, M. A., & Helmich, R. C. (2020). Systematic clinical approach for diagnosing upper limb tremor. Journal of neurology, neurosurgery, and psychiatry, 91(8), 822–830. https://doi.org/10.1136/jnnp-2019-322676
- Crawford, P., & Zimmerman, E. E. (2018). Tremor: Sorting Through the Differential Diagnosis. American family physician, 97(3), 180–186.
- Vijiaratnam, N., Wirth, T., & Morris, H. R. (2020). Revisiting the assessment of tremor: clinical review. The British journal of general practice : the journal of the Royal College of General Practitioners, 70(701), 611–614. https://doi.org/10.3399/bjgp20X713849
- Alty, Jane & Kempster, Peter. (2011). A practical guide to the differential diagnosis of tremor. Postgraduate medical journal. 87. 623-9. 10.1136/pgmj.2009.089623.