Allergic rhinitis
Allergic Rhinitis
The most common form of non-infectious rhinitis.
Caused by an IgE-mediated immune response to allergens.
Often accompanied by ocular symptoms (e.g. itchy or watery eyes).
Pathophysiology
Primarily driven by IgE-mediated immune responses.
- When exposed to allergens in the environment, allergen-specific IgE is produced which attaches to FcεRI on mast cells & basophils –> release of mediators (histamine, leukotrienes & others) –> allergic response.
The allergic response is biphasic, with an early phase of nasal pruritus, itching, rhinorrhea, & a late phase with predominant nasal congestion.
Non-IgE-mediated mechanism may also have a role but its significance is undetermined and requires further investigation/studies.
Classification
Allergic rhinitis (AR) is traditionally classified into:
- Seasonal: Triggered by outdoor allergens like pollens
- Perennial: Caused by indoor allergens such as house dust mites, animal danders, cockroaches & molds.
Shortcoming of the traditional classification
- Overlap of allergens: Some pollens/molds are present year-round
- Variable symptoms: Perennial allergens don’t always cause year-round symptoms
- Polysensitization: Most patients react to multiple allergens across seasons
- Environmental factors: Climate change and travel affect exposure
- Irritants: Pollution and other nonallergic triggers worsen symptoms
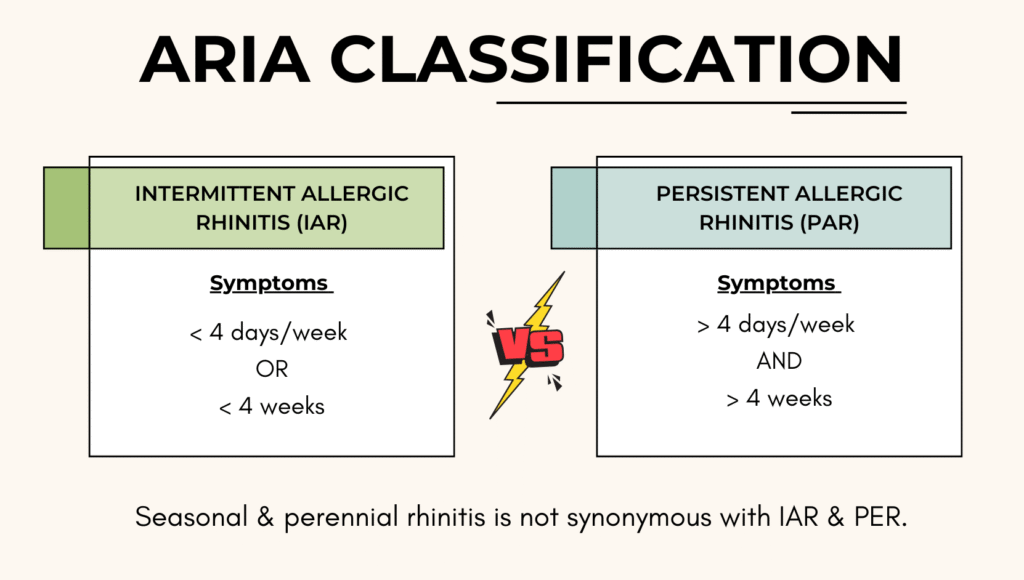
In view of these, ARIA has came out with another classification which divide allergic rhinitis into intermittent & persistent based on duration of symptoms occurrence.
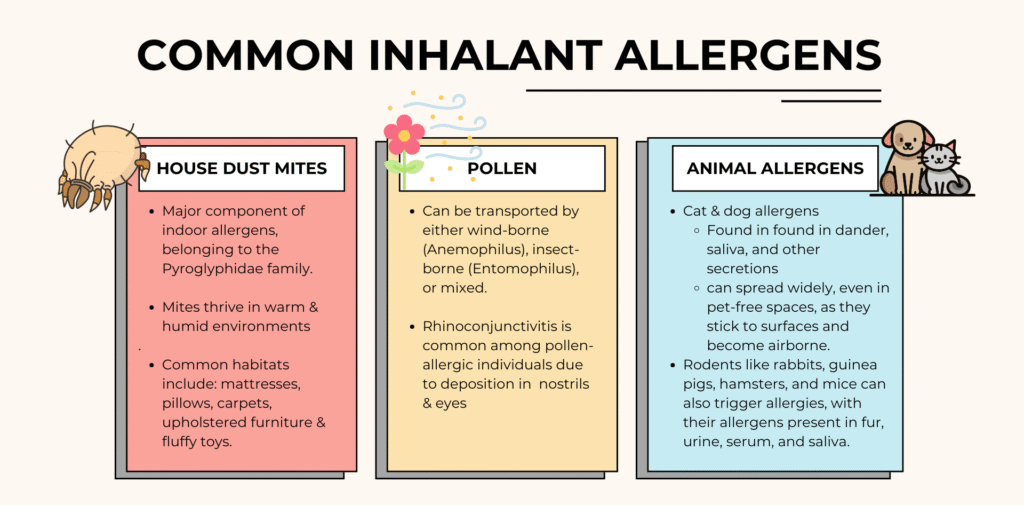
Inhalant Allergens (Aeroallergens)
Major contributors to allergic rhinitis.
Can be categorized as:
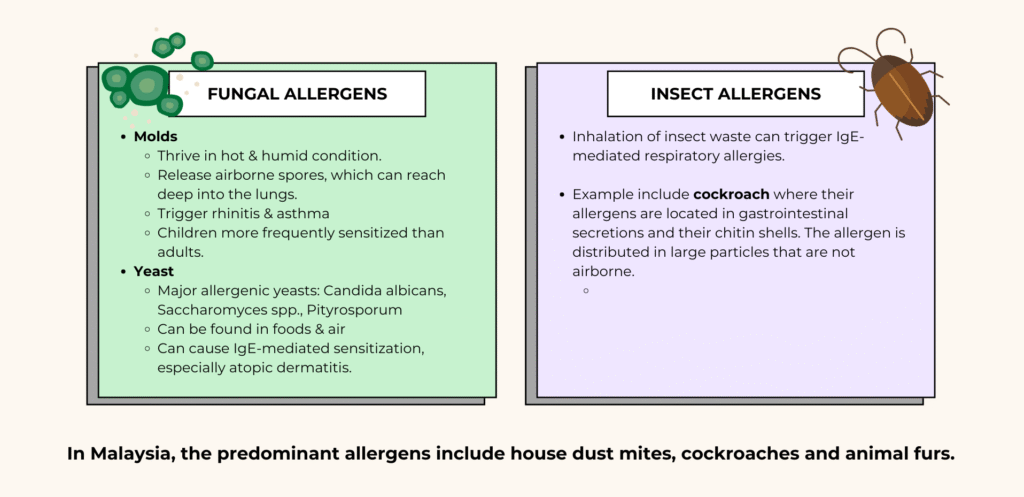
- Indoor – mites, pets, insects, indoor molds
- Outdoor – pollens, outdoor molds
- Occupational – workplace-specific allergens
Diagnosis
Diagnosis of allergic rhinitis depends on typical history + diagnostic tests
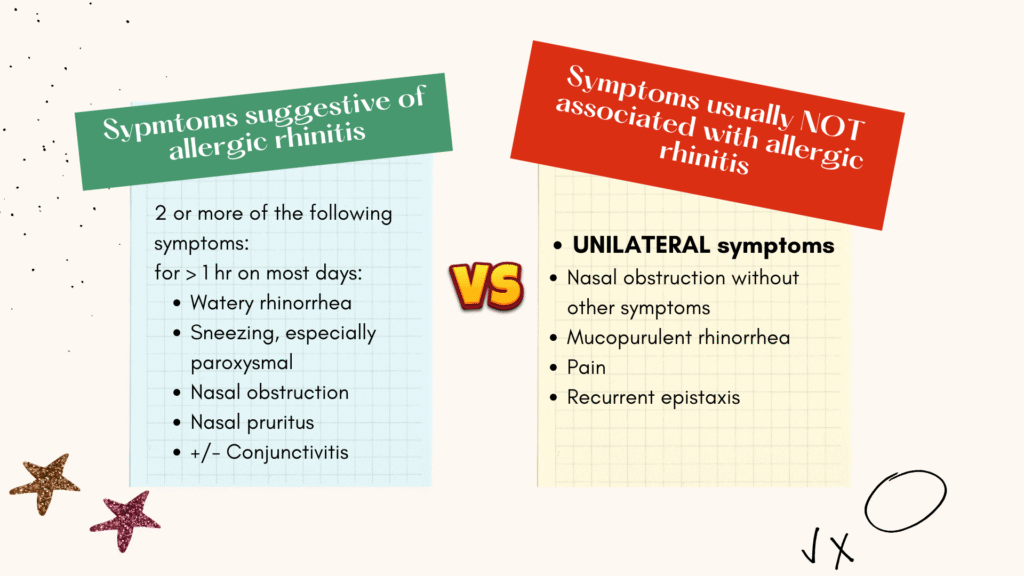
Typical symptoms include:
- Rhinorrhea
- Sneezing
- Nasal obstruction
- Pruritus
- Ocular symptoms are commonly associated especially for those allergic to outdoor allergens
Diagnostic tests
1. Skin tests
Demonstrates IgE-mediated hypersensitivity.
Among the various methods available, Skin Prick Test is the recommended.
Drugs that can interfere with test results (including but not limited to) :
- Oral H1-antihistamines
- Imipramines (Tricyclic antidepressants)
- Phenothiazines (Antipsychotic)
- Topical steroids
- Possibly oral corticosteroids
Montelukast does not interfere with results & do not need to be discontinued before test.
2. Blood test – Serum allergen-specific IgE
Total serum IgE not recommended: non specific; can be raised in allergy, parasitic disease & other conditions)
Serum allergen-specific IgE:
- Correlates closely to skin test & nasal challenges
- Less sensitive than skin prick test.
- Positive cut-of: ≥0.35 KU/L, but some sensitized patients may test below this.
- IgE level does not predict symptoms severity, where in fact the clinical symptoms depend on multiple factors beyond IgE concentration alone.
3. Nasal challenge test
Mostly used in research, & to lesser extent, in clinical practice.
However it has a role mainly in diagnosis of occupational rhinitis.
4. Other investigations
Nasal endoscopy – to visualize the posterior nasal cavity & the middle meatus.
Imaging
- Plain sinus radiographs are not indicated
- CT is not routinely done, but can be considered:
– To eliminate other conditions.
– To exclude chronic rhinosinusitis if indicated
– To assess for any rhinitis complications
– In patients who do not respond to treatment
– In patients with unilateral rhinitis - MRI may only be useful if fungal sinusitis, tumors & encephaloceles are suspected.
General Diagnostic Workflow
Skin prick test is often the preferred 1st line diagnostic methods.
- If results match clinical history: no further testing usually needed
- If results do not match clinical history: serum IgE & sometimes nasal challenges can help with further assessment.
In general practice, though, skin tests are not routinely available, and serum specific IgE are used instead.
Severity classification
Assessment of severity can help guide treatment and assess treatment response.
This can be done using either the ARIA classification or the Visual Analogue Score (VAS)
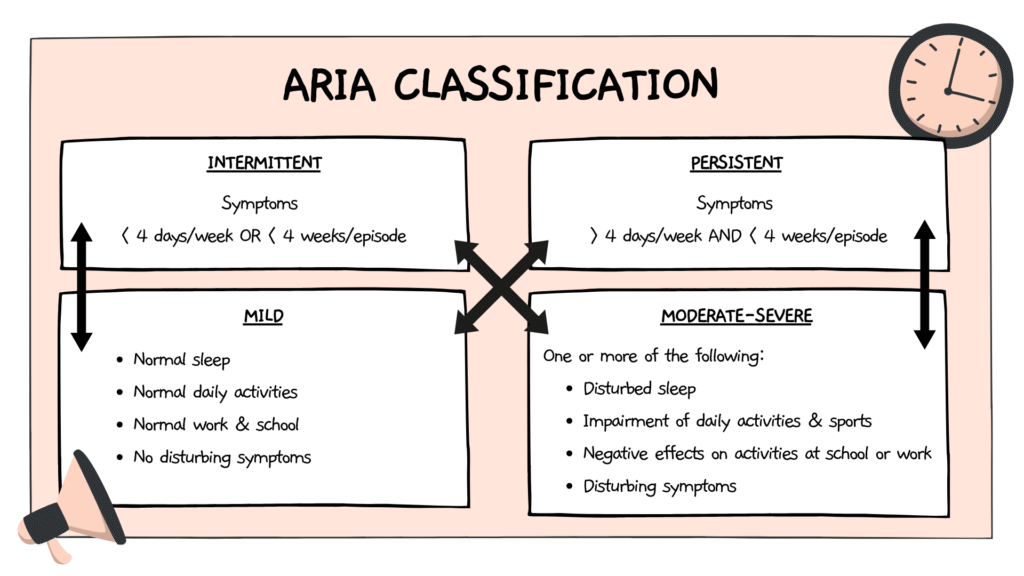
ARIA
Mild
- Normal sleep
- No negative effects on everyday activity, sports, leisure
- Normal functioning at school or work
- No troublesome symptoms
Moderate/Severe
One or more items :
- Disturbed sleep
- Negative effects on everyday activity, sports, leisure
- Negative effects on activities at school or work
- Troublesome symptoms
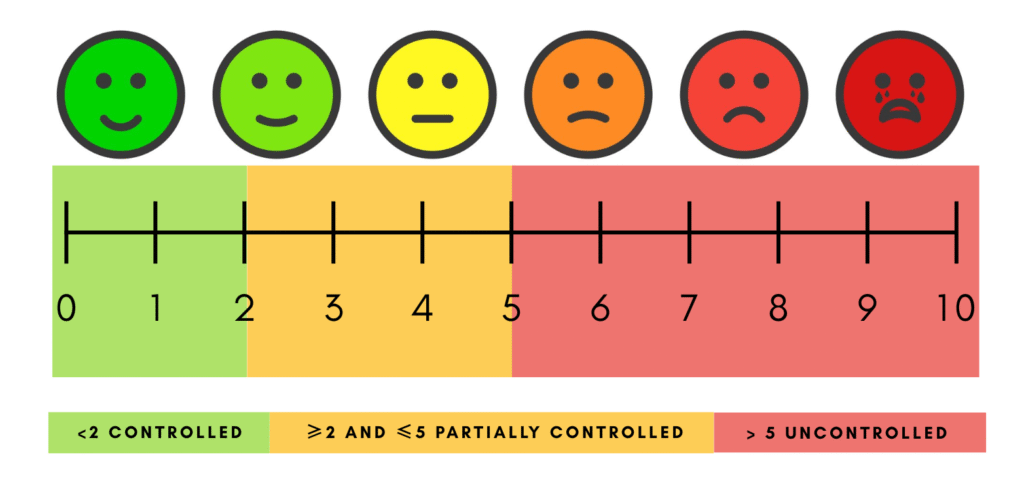
Visual Analogue Scale (VAS)
Management
The management of Acute Rhinitis (AR) consists of :
- Patient education – ensuring patient understand the nature of the disease, allergen avoidance, treatment options, and self-care strategies.
- Pharmacotherapy – including antihistamines, intranasal corticosteroids, & other appropriate medications tailored to symptom severity.
- Allergen-specific immune therapy – considered in patients with persistent symptoms despite pharmacological treatment or where long-term disease modification is desired.
Role of environmental control
While allergen avoidance is expected to improve symptoms, evidence to support the effectiveness of single physical or chemical methods is limited.
- Mattress encasing or HEPA filter when used alone shows little benefit & their effects are inconclusive.
- Animal allergen avoidance at home may help, though exposure in public spaces remains unavoidable.
Multifaceted avoidance intervention may be helpful for some highly-selected patients after environmental counselling.
Examples of avoidance measures
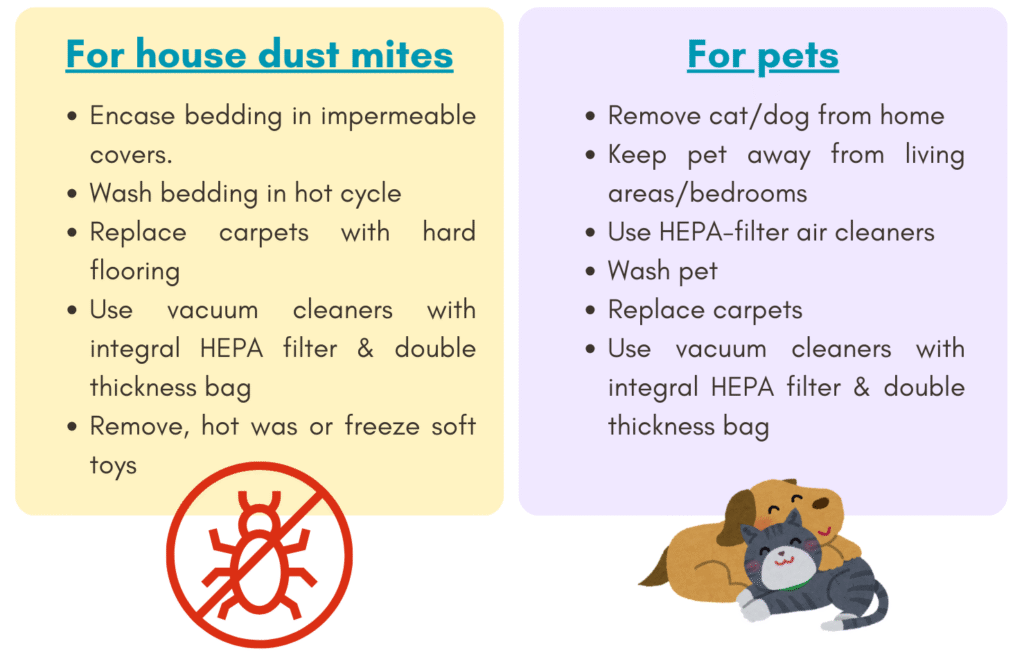
Note: While these measures may be helpful, strong evidence for consistent clinical benefit is lacking.
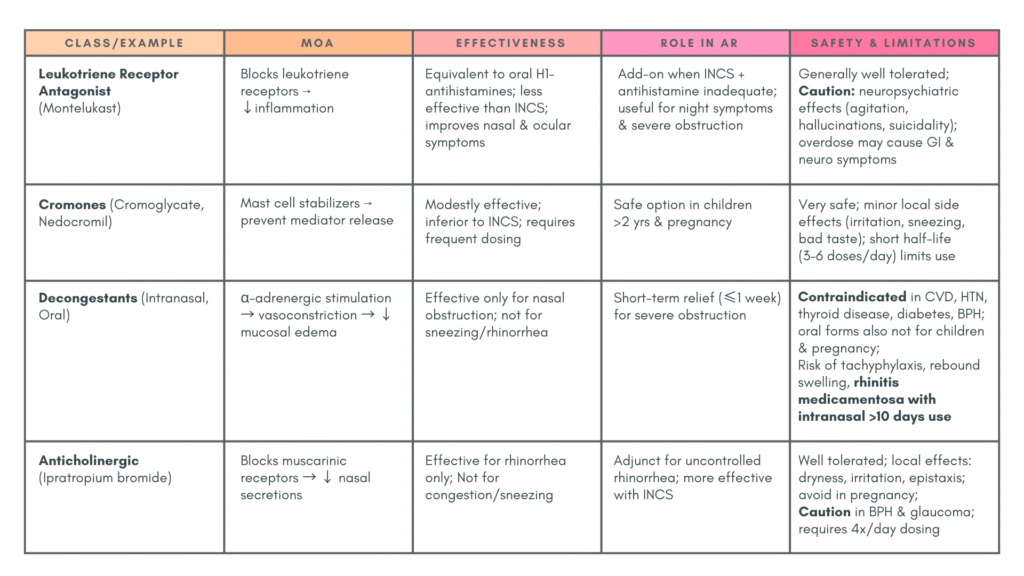
Pharmacotherapy
Generally consists of :
- H1– Antihistamine – Oral/Intranasal
- Intranasal corticosteroids (INCS)
- Adjuvant/add-on therapy: Leukotriene receptor antagonist (Montelukast), Intranasal/oral decongestants, Intranasal ipratropium
Key points
- Among these, intranasal glucocorticoids had been found to be the most effective.
- The effects of these medications are generally not sustained after stopping; maintenance treatment is often needed especially in PER.
- Tachyphylaxis does not occur with prolonged treatment.
- Treatment response should be reassessed after 2 weeks to decide whether to maintain, step up or step down therapy.
1) H1– Antihistamine
Oral H1– Antihistamine
Effectiveness
- Relieves histamine-mediated symptoms: rhinorrhea, sneezing, nasal itching & eye symptoms
2nd generation are recommended over the 1st generation due to their favorable efficacy/safety ratio.
Long term treatment is safe.
Can be used as 1st line for mild-to-moderate AR.
Can also be used with intranasal corticosteroids (INCS) for moderate-to-severe AR or refractory symptoms.
Intranasal Antihistamine
Effective in reducing itching, sneezing, runny nose & nasal congestion.
Provide faster relief of nasal congestion compared to oral antihistamines.
Generally well tolerated.
Can be used with intranasal corticosteroids (INCS-INA combination) for :
- Moderate-to-severe AR
- Refractory symptoms
- Faster symptom resolution
Note: INCS-INA combination offers better clinical impact than INCS + oral antihistamines.
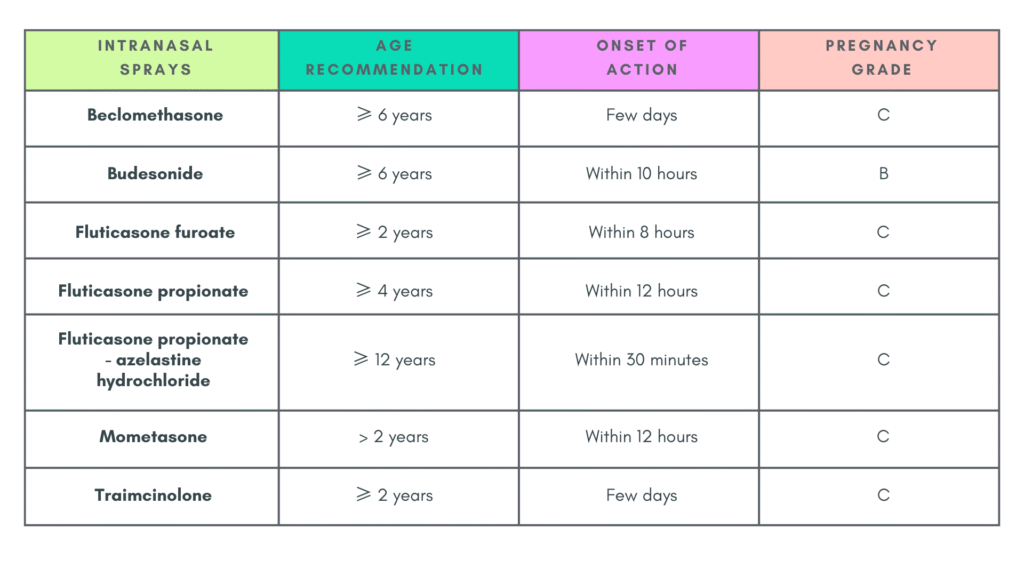
2) Intranasal corticosteroids (INCS) 🌟
Most effective monotherapy for AR & is safe for long term use.
Role in AR management
- Effective in against both early & late inflammatory response, improving all symptoms of AR.
- Considered the 1st line if nasal congestion is present or symptoms are frequent.
- Superior to oral antihistamines for nasal symptoms; also improves ocular symptoms & lower airway symptoms when there is concomitant allergic conjunctivitis & asthma.
- Indicated in mild, moderate, & severe AR.
- Can be used as 1st line as an alternative to 2nd gen oral antihistamine.
- Combination with INA = better control in severe/refractory AR
Onset
- Optimal effect: within 1 – 2 weeks of consistent use.
- Long term control may require maintenance therapy with INCS or INCS-INA for months to year.
Safety & Tolerability
- Well-tolerated and safe, with negligible systemic absorption.
- Local side effect may include: burning, epistaxis, nasal dryness, crusting, throat irritation & bitter aftertaste.
- No conclusive evidence of growth suppression in children with up to 1 year of use.
- While generally not linked to a significant risk of increased intraocular pressure (IOP) or cataracts, there is a potential risk of IOP for patients with pre-existing glaucoma. Therefore, it is advisable to avoid use in individuals with underlying glaucoma.
3) Adjuvant/add-on therapy
Allergen-specific immunotherapy
Can be considered for patients refractory to optimal medical therapy (INCS + oral antihistamine)
What it is
- Involves the gradual administration of increasing doses of an allergen extract.
- Aim: to reduce symptoms on future exposure by inducing clinical & immune tolerance.
Efficacy & benefits
- Effective treatment for allergic rhinitis & asthma
- Provides long-term efficacy, even after discontinuation (provided the duration of therapy is at least 3 years)
- Improves QoL.
- Can help prevent progression of allergic disease –> reduce development of asthma in AR patients (secondary prevention of asthma)
Route of administration
- Subcutaneous immunotherapy (SCIT)
– Effective for both rhinitis & asthma
– Benefits may persist year after cessation.
– There are risk of systemic side effects ranging from mild to severe including anaphylaxis. - Sublingual immunotherapy (SLIT)
– Available as drops or tablets.
– Recommended for pollen allergy & may be used for mite allergy.
– Safer with less risk of systemic adverse effects.
Requirements before starting: Confirmation of IgE-mediated allergy with positive skin prick test &/or elevated allergen-specific IgE
Surgical treatment
Does not treat the allergic disease itself.
May only be used in certain conditions like :
- Turbinate hypertrophy
- Cartilaginous or bony obstruction of the nasal airways
- Secondary & independent sinus disease
Nasal & sinus surgery should only be considered when adequate medical treatment fails & when the anatomical variation or disease has clear functional & clinical significance.
Summary of approach to treatment
- Diagnosis of allergic rhinitis – typical history + diagnostic tests
- Severity assessment – ARIA or VAS
- Treat according to severity
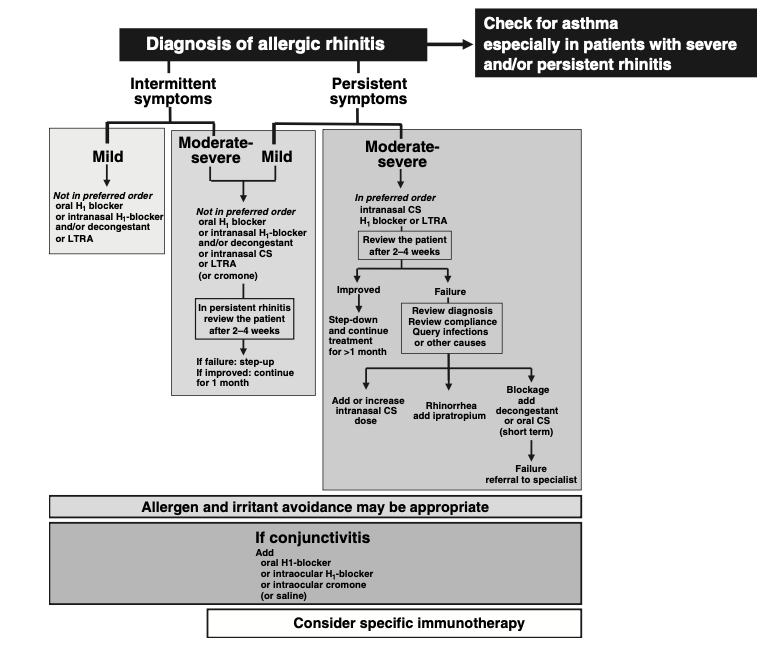
Approach using the ARIA classification
Approach using VAS
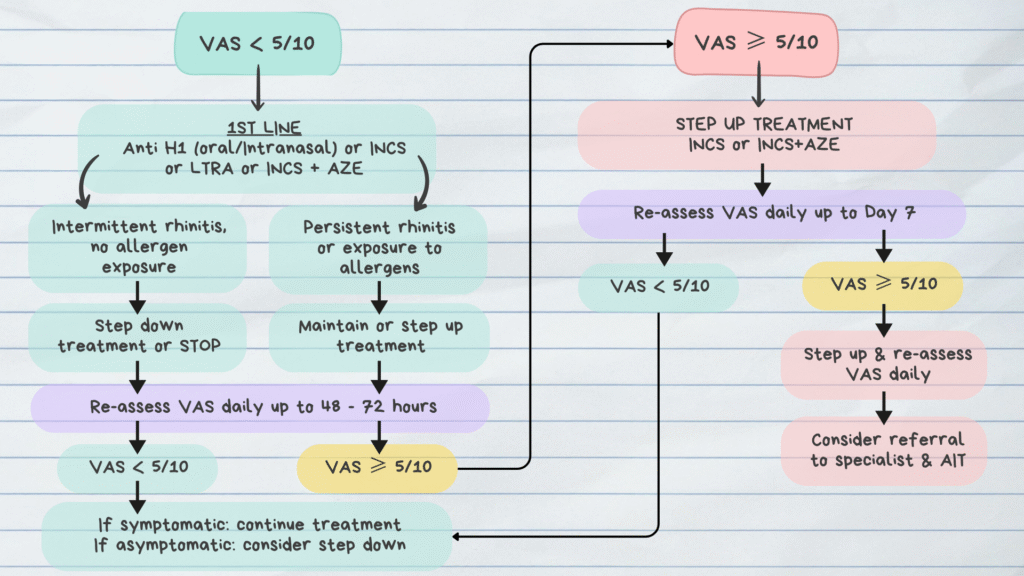
Anti H1: Antihistamine; INCS: Intranasal corticosteroids; LTRA: Leukotriene receptor antagonists;
INCS+AZE: Intranasal corticosteroids + Intranasal antihistamines
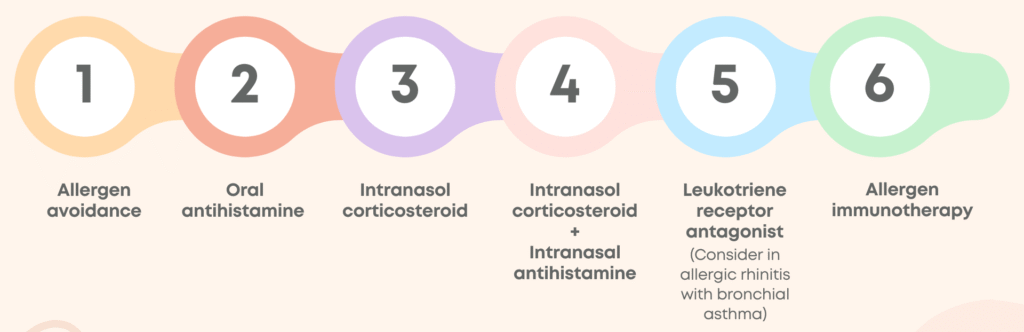
General treatment approach
The diagram below represents a simplified treatment approach if both of the above seems a bit robust.
References
- Bousquet J, Khaltaev N, Cruz AA, Denburg J, et al; World Health Organization; GA(2)LEN; AllerGen. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008 Apr;63 Suppl 86:8-160. doi: 10.1111/j.1398-9995.2007.01620.x. PMID: 18331513.
- Abdullah B, Abdul Latiff AH, Manuel AM, et al. Pharmacological Management of Allergic Rhinitis: A Consensus Statement from the Malaysian Society of Allergy and Immunology. J Asthma Allergy. 2022;15:983-1003 https://doi.org/10.2147/JAA.S374346
- Abdul Latiff AH, Husain S, Abdullah B, et al. ARIA Care Pathways 2019: Next-Generation Allergic Rhinitis Care and Allergen Immunotherapy in Malaysia. J Pers Med. 2023 May 15;13(5):835. doi: 10.3390/jpm13050835. PMID: 37241005; PMCID: PMC10222413.