Acute bronchiolitis

Acute Bronchiolitis
Epidemiology
Age group: Affects infants and children <2 years, most commonly in the 1st year of life, peaking between 3 – 6 months.
Common causative agent: Respiratory Syncytial Virus (RSV)
Other possible viral agents: Adenovirus, Influenza virus, Parainfluenza virus, Metapneumovirus
Clinical presentation
a) Coryzal prodrome (1 – 3 days) – rhinorrhea, mild cough
b) Followed by lower respiratory tract involvement, presenting as:
- Persistent cough AND
- Tachypnoea ± chest recession (or both) AND
- Wheeze ± crackles on auscultation (or both)
c) Some associated symptoms may be present:
- Fever (usually < 39 oC)
- Poor feeding (typically after 3 – 5 days of illness)
d) Look out for signs of impending respiratory failure:
- Signs of exhaustion, e.g. listlessness or decreased respiratory effort
- Recurrent apnea
- Failure to maintain oxygen saturation despite oxygen supplementation
In young infants especially < 6 weeks, they may present with apnea as the only symptom/sign
Course of illness: Symptoms usually peak at days 3 – 5, & cough resolve in ~90% of infants within 3 weeks.
Key safety information for parents
1. Recognizing “red flag 🚩” symptoms
- Worsening work of breathing (e.g. grunting, nasal flaring, marked chest recession)
- Fluid intake is 50 – 75% of normal and no wet nappy for 12 hours.
- Apnea or cyanosis
2. Avoid smoking in the baby/child’s home –> can increase the risk of more severe symptoms
3. Get help immediately if “red flag” symptoms are present.
Differential diagnosis
Bronchiolitis is primarily a clinical diagnosis, but several conditions can mimic its presentation. Key alternative diagnoses to consider include:
i. Pneumonia
Consider pneumonia as a possible diagnosis if there are features of :
- High fever (typically > 39 oC)
- Persistent focal crackles on auscultation.
ii. Viral-induced wheeze/Early childhood asthma (in older infants & young children)
More likely when there is:
- Persistent wheeze without crackles OR
- Recurrent episodic wheeze OR
- A personal or family history of atopy
Investigations
Blood tests and CXR are not routinely indicated. CXR changes may be misleading, as they can mimic pneumonia and may lead to unnecessary use of antibiotics.
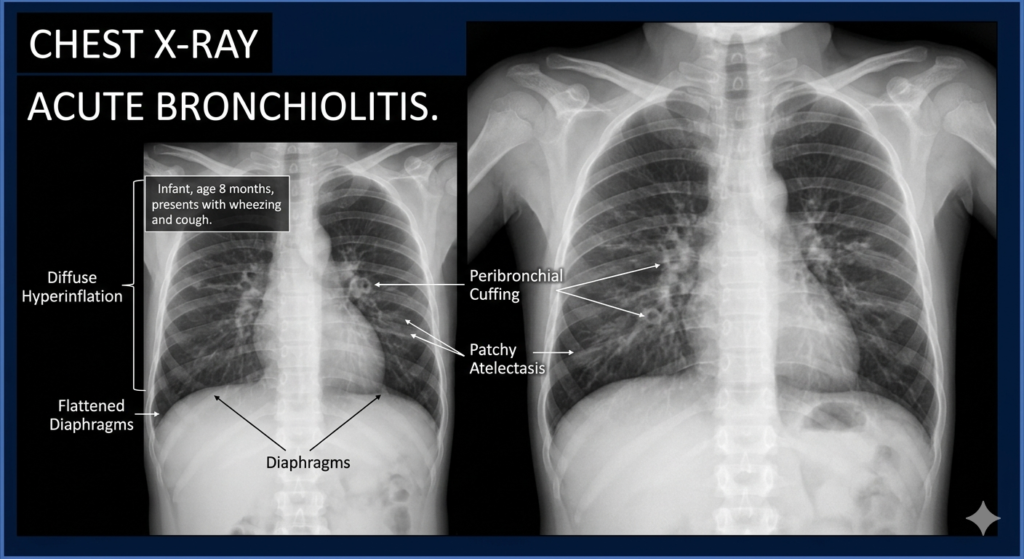
Possible CXR changes include :
- Hyperinflation (most common)
- Segmental collapse/consolidation
- Lobar collapse/consolidation.
Consider CXR if :
- Severe respiratory distress
- Unusual clinical features
- Any underlying cardiac or chronic respiratory disorder
- Admission to intensive care
Management
1. Supportive care is the mainstay.
2. Airway clearance
2.1 Chest physiotherapy
- Not routinely recommended.
- May be considered in children with impair secretion clearance, e.g.
– Spinal muscular atrophy
– Severe tracheomalacia
2.2 Upper airway suctioning
- Consider if there is :
– Respiratory distress or feeding difficulty due to upper airway secretions
– Apnea, even when secretions are not obvious.
3. Oxygen Therapy
Give supplemental oxygen if oxygen saturation is :
- Persistently < 90% in children aged ≥ 6 weeks.
- Persistently < 92% in :
– Infants < 6 weeks
– Children of any age with underlying health conditions
4. Respiratory support
- Consider CPAP if there are signs of impending respiratory failure
5. Hydration & feeding
- Enteral fluids (via nasogastric or orogastric tube) if the child cannot maintain adequate oral intake.
- Intravenous fluids if
– NG/OG feeding is not tolerated
– There is impending respiratory failure
Treatments that are not routinely recommended :
- Antibiotics
- Nebulized adrenaline
- Salbutamol
- Montelukast
- Ipratropium bromide
- Systemic or inhaled corticosteroids
Regarding hypertonic saline
- Not routinely recommended by NICE guideline.
- However, Malaysian Pediatric Protocol (4th edition) note that it may improve clinical severity scores in both outpatients & inpatients, thus may be considered.
- A Cochrane systemic review by Zhang, L. et al. found that hypertonic saline may modestly reduce length of stay in hospitalized infants and may also slightly improve clinical severity score, though the strength of the evidence was low to very low.
Home vs Hospital management
Role of primary care as first point of contact is to assess whether the child is suitable for home management or should be referred to the hospital.
The table below serves as a guideline in our assessment

High risk group includes those with:
- Chronic lung disease (including bronchopulmonary dysplasia)
- Hemodynamically significant congenital heart disease
- Age in young infants (< 3 months)
- Premature birth, especially < 32 weeks
- Neuromuscular disorders
- Immunodeficiency
Other factors to consider:
- Social circumstances
- Skill & confidence of the care in looking after the child
- Confidence in being able to spot red flag symptoms
- Distance to healthcare in case of deterioration
References
- Shawn L. Ralston, Allan S. Lieberthal, H. Cody Meissner, et al; Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis. Pediatrics November 2014; 134 (5): e1474–e1502. 10.1542/peds.2014-2742
- Bronchiolitis in children: diagnosis and management. London: National Institute for Health and Care Excellence (NICE); 2021 Aug 9. (NICE Guideline, No. 9.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK573086/
- Ministry of Health Malaysia. (2018). Paediatric protocols for Malaysian hospitals (4th ed.). Malaysian Paediatric Association.
- Zhang, L., Mendoza-Sassi, R. A., Wainwright, C. E., Aregbesola, A., & Klassen, T. P. (2023). Nebulised hypertonic saline solution for acute bronchiolitis in infants. The Cochrane database of systematic reviews, 4(4), CD006458. https://doi.org/10.1002/14651858.CD006458.pub5