Childhood asthma exacerbation

Childhood Asthma Exacerbation
Clinical features
Asthma exacerbations (or asthma attacks) are episodes characterized by gradual increase in symptoms such as shortness of breath, cough, wheezing and chest tightness, or a combination of these symptoms. They are also associated with a progressive decline in lung function, represented by a significant change from the patient’s usual condition that necessitates a change in treatment.
Early symptoms of exacerbation in young children may include:
- Increased symptoms (wheeze & shortness of breath)
- Increased coughing (especially at night)
- Lethargy or reduced exercise tolerance
- Impaired daily activities including feeding
- Poor response to reliever medication
In children aged 2–5 years, a combination of increased daytime cough, daytime wheezing, and nighttime use of β2-agonists was found in a study to strongly predict an impending asthma exacerbation at the group level, typically occurring one day later.
Viral upper respiratory tract infections (URTIs) are common triggers of asthma exacerbations in many, though not all, children with asthma.
Assessment of clinical severity
It is important to assess the severity of exacerbation as it will guide the necessary treatment and referral whenever indicated.
Some of the important signs that indicate a severe exacerbation:
- O2 saturation (pulse oximetry)
– < 92% on presentation (before oxygen or bronchodilator treatment) is associated with high morbidity & likely need for hospitalization.
– Saturation of 92 – 95% is also associated with higher risk. - Signs of cerebral hypoxemia – Agitation, drowsiness & confusion
- Quiet chest on auscultation – indicates minimal ventilation, insufficient to produce a wheeze.
There are few Clinical Scoring Systems that can be used to classify the severity of exacerbations – Pediatric Asthma Score (PAS), Pediatric Asthma Severity Score (PASS), Preschool Respiratory Assessment Measure (PRAM).
PAS is used in our Malaysia CPG Management of Childhood Asthma 2024 consensus statement (4th edition)
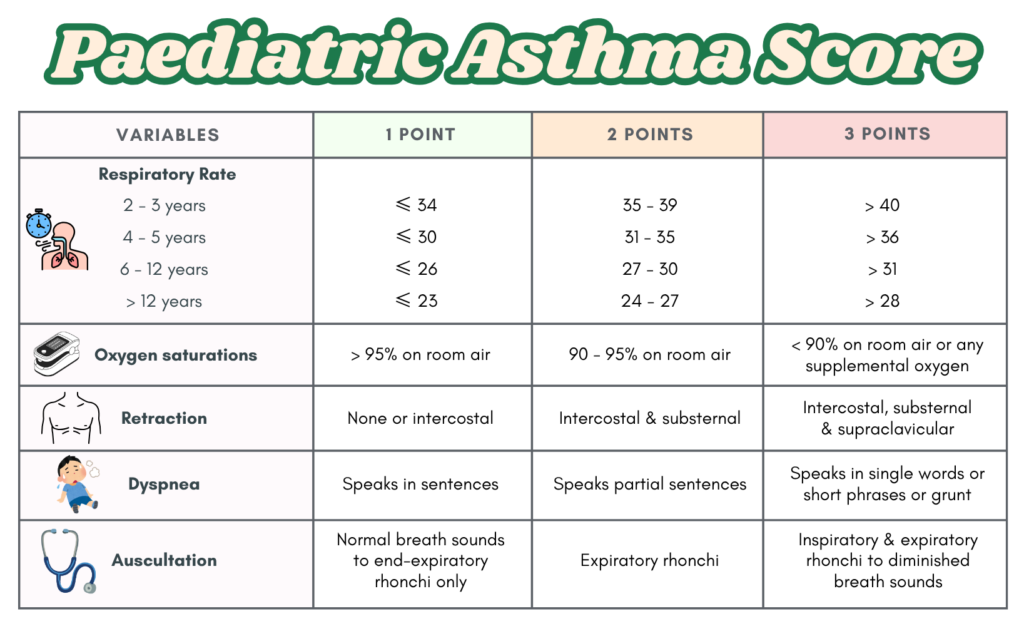
Used in child aged 2 – 18 years old to assess exacerbation severity
Treatment of acute exacerbations
First-line for standard therapy: SABA, SAMA, Corticosteroids, Controlled/titrated oxygen therapy
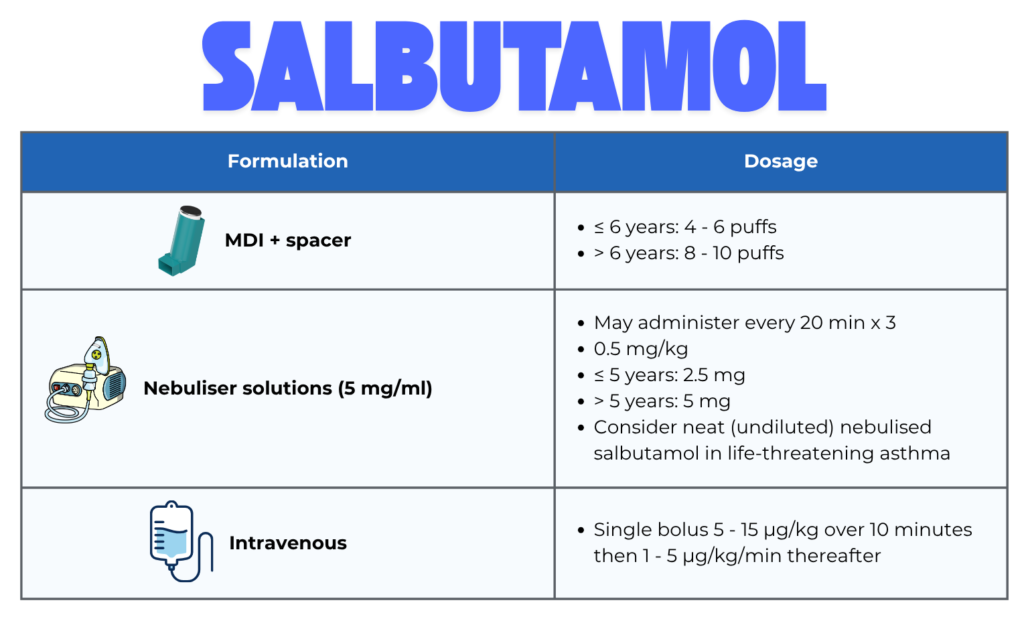
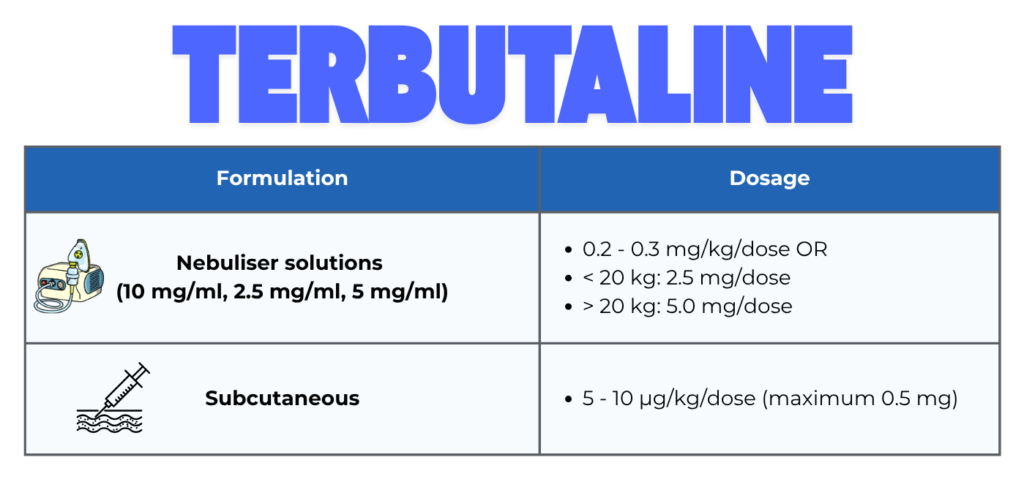
A. Short acting B2- agonist (SABA) – First line
- Bronchodilator of choice
- pMDI with spacer (preferred in children over nebulized in mild-moderate exacerbation) as it is more efficient than nebulizer for bronchodilator delivery.
- In severe & life-threatening cases, oxygen-driven nebulized SABA + SAMA (ipratropium) combination is recommended.
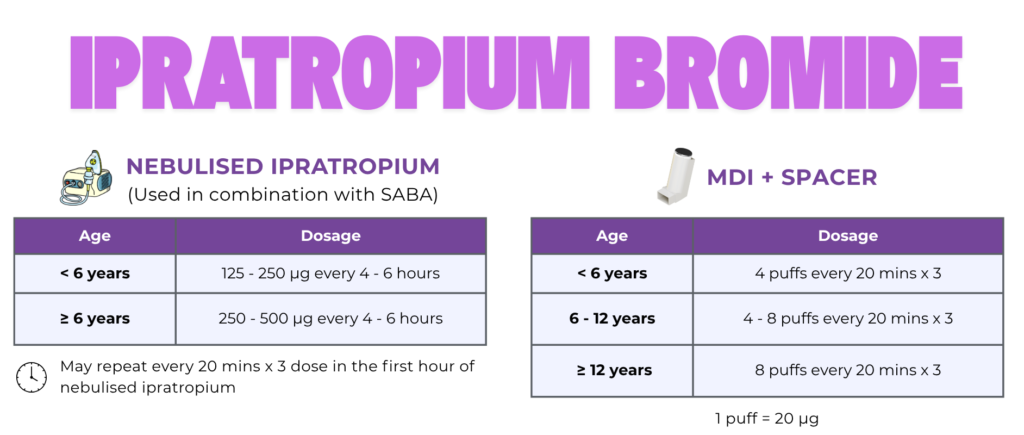
B. Short acting muscarinic antagonist (SAMA) – Ipratropium Bromide (Add on)
When to add?
- If symptoms are refractory to initial SABA treatment.
- In moderate, severe of life-threatening exacerbations
It has limited role in moderate asthma exacerbation as it has minimal effect on hospital admissions & potential increased risk of adverse events (Risk may be > benefit).
Dosing:
- Every 20 – 30 mins (in addition to SABA) during the first hour, may be continued up to max of 2 hours.
- Then stop or taper to 4 – 6 hourly
Precaution: Use a well-fitted mask during nebulization to avoid contact with the eyes.
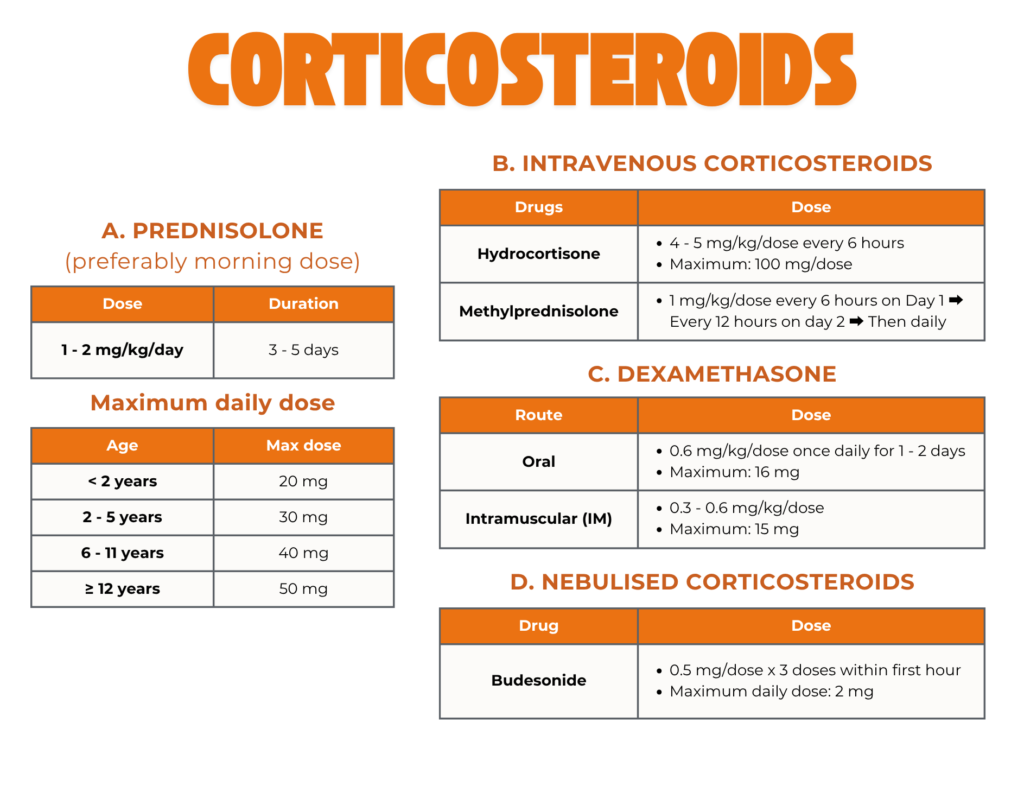
C. Corticosteroids – oral, parenteral or nebulized
Give early, within one hour to hasten recovery.
Oral route is preferred – quicker, less expensive & less invasive.
Parenteral route – for children who are vomiting or unable to tolerate orally & in severe or life-threatening exacerbations.
Oral & parenteral corticosteroids need at least 4 hours to produce clinical improvement.
Duration of treatment :
- Children : 3 – 5 days
- Adolescent (≥ 12 years) : 5 – 7 days
Weaning is unnecessary if the course is < 14 days.
Nebulized corticosteroids
- Consider neb corticosteroids + SABA + SAMA every 20 mins during the 1st hour in severe exacerbations.
- Theoretical advantages of nebulized steroids :
– Faster onset of action (1 – 2 hours vs 4 hours)
– More localized airway effects – reduces bronchial mucosal swelling & bronchospasm
– Less systemic side effects
D. Controlled/Titrated Oxygen Therapy
Start oxygen therapy if :
- SpO2 < 94% (GINA 2026 recommends lower threshold < 92%) OR
- In severe/life-threatening exacerbations
Target : Maintain SpO2 94 – 98% (GINA 2026 target SpO2 > 92%)
Key points :
- In acutely distressed patients, use oxygen-driven nebulized bronchodilators.
- Continuous SpO2 monitoring is important (desaturation may occur during sleep)
Consider early respiratory support with HFNC or NIV in severe acute asthma.
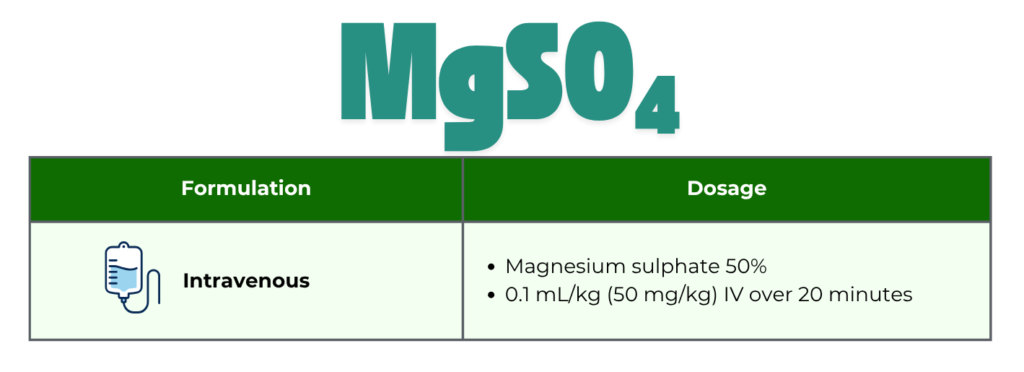
E. IV Magnesium Sulphate (IV MgSO4)
Role : Consider as first line option for adjunct/second-line IV treatment of severe or life-threatening exacerbation.
Key points : Safe & beneficial in severe asthma, may be considered in addition to the standard treatment (salbutamol + ipratropium + OCS), after the first hour of treatment for children ≥ 2 years old.
Treatments that are not recommended for acute exacerbations ❌ :
- Antibiotics – unless concurrent pneumonia or other bacterial infections suspected.
- IM adrenaline – administer only if associated with anaphylaxis & angioedema
- Sedatives – can cause drowsiness & hypoventilation/apnea
- Mucolytics – may worsen cough
- Nebulized hypertonic saline – may cause bronchoconstriction
- Chest physiotherapy – May cause discomfort & bronchospasm
Regarding Chest X-ray
Not routinely recommended.
Consider if :
- Suspected pneumothorax/pneumomediastinum (i.e. presence of subcutaneous emphysema)
- Lung collapse or consolidation needs to be ruled out
- Poor response in life-threatening asthma
- Ventilation required
- Suspected foreign body inhalation.
Management of exacerbation using PAS score
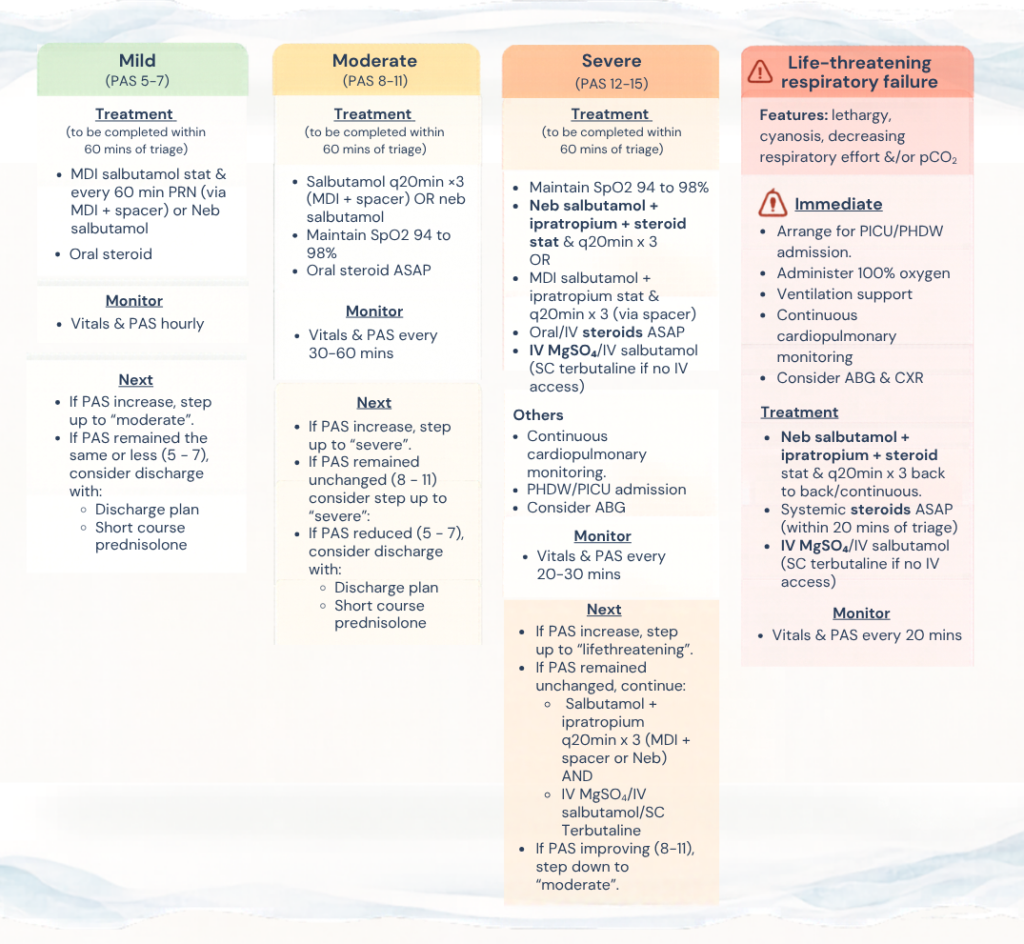
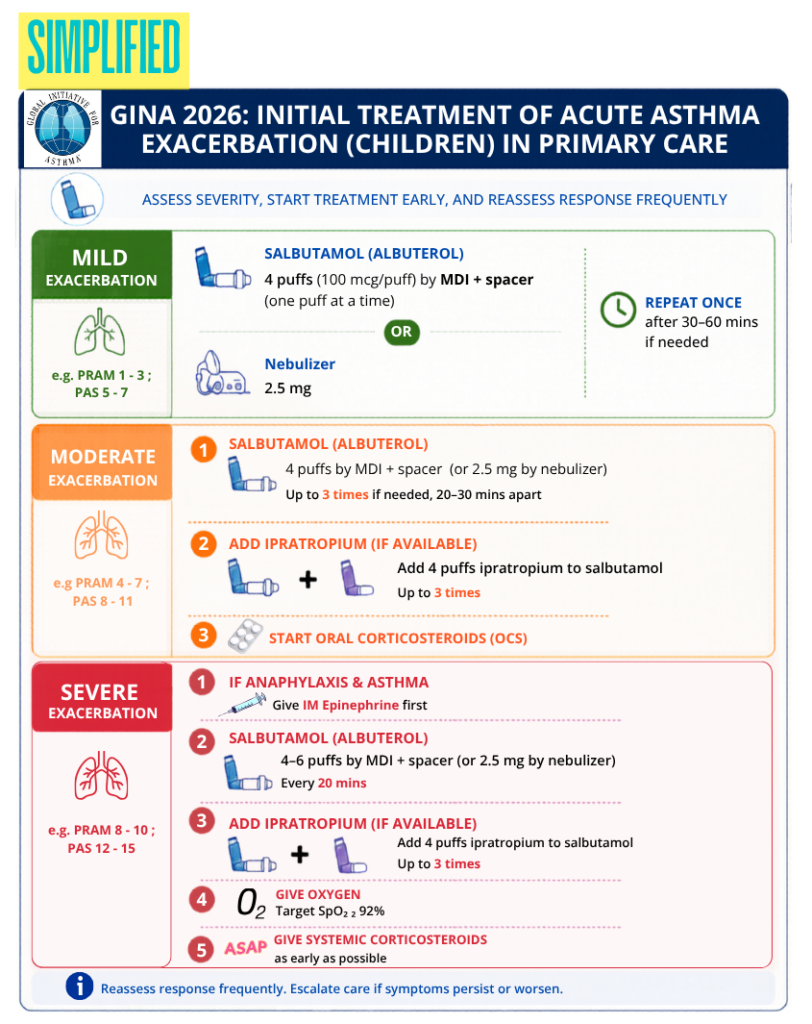
GINA 2026 recommendation
Mild exacerbations
- 4 puffs salbutamol (albuterol) 100 mcg/puff by spacer (one puff at a time) OR 2.5 mg by nebulizer.
- Repeat once after 30 – 60 mins if needed
Moderate exacerbations
- 4 puffs salbutamol by MDI + spacer (or 2.5 mg by nebulizer) up to 3 times if needed, 20 – 30 mins apart
- ADD 4 puff ipratropium (if available) to salbutamol for up to 3 times.
- Start oral corticosteroids (OCS)
Severe exacerbations
- If anaphylaxis & asthma, given IM epinephrine first.
- 4 – 6 puffs salbutamol by MDI + spacer (or 2.5 mg by nebulizer), every 20 mins.
- ADD 4 puff ipratropium (if available) to salbutamol for up to 3 times.
- Give oxygen: target SpO2 ≥ 92%
- Give systemic corticosteroids.
Discharge & follow up after an exacerbation
Discharge criteria in primary care
- Clinical status : Symptoms & signs improved for at least 1 – 2 hours after last salbutamol dose.
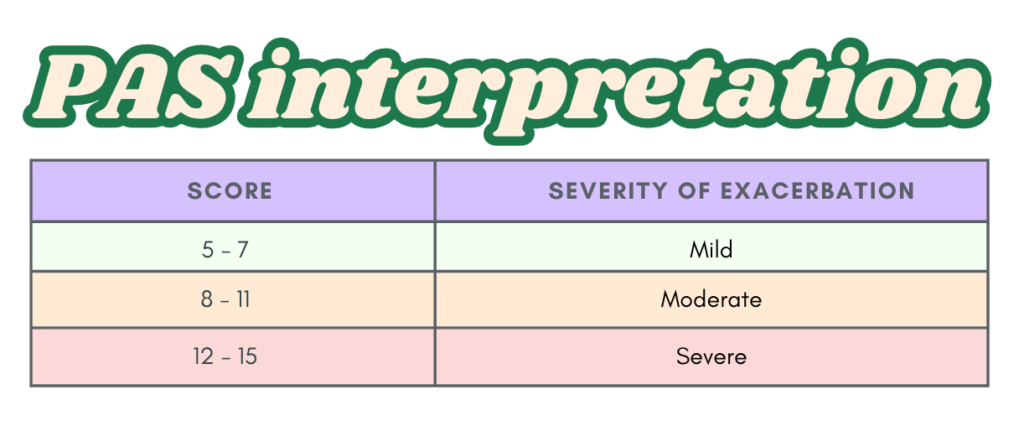
- Pediatric asthma score (PAS) : ≤ 7 (achieved ‘mild’ criteria)
- Oxygenation : SpO2 > 94% in room air (GINA 2026 > 92%)
- Lung function (if available) : Post-bronchodilator PEV &/or FEV1 should be > 70% of best or predicted values
Arranging for follow up :
- At primary care – within 2 weeks (or earlier) with a written asthma action plan.
(GINA 2026 recommends follow up within 1 – 3 days, then next within 2 – 3 months) - At pediatric asthma clinic within 1 – 2 months
- Referral to pediatric respiratory specialist if it was a life-threatening exacerbation.
Follow up should aim to :
- Ensure complete recovery.
- Identify the trigger/cause of exacerbation
- Establish appropriate maintenance treatment (when necessary)
- Assess adherence & inhaler technique (if started)
Essential discharge counselling (before going home)
A. Recognizing worsening asthma.
Parents/carers should know :
- Early warning signs of deterioration
- Recurrence symptoms
- Trigger identification & avoidance strategies
B. Asthma action plan (AAP) : Provide a clear, written individualized AAP.
C. Review inhaler technique
D. Appropriate SABA use
- Use PRN only. Avoid excessive reliance on SABA that may mask worsening asthma.
- Monitor : Daily SABA requirement should gradually return to pre-exacerbation level.
E. Controller medication
- Confirm that ICS has been started (if the child had presented with moderate or severe exacerbation) or continued where appropriate.
- Suggested approach after discharge : Twice the low initial ICS dose for the first month, then titrate accordingly.
F. Medication supply
Ensure adequate supply of :
- SABA reliever
- Remaining oral corticosteroid course (if prescribed)
– Prednisolone total 3 – 5 days
– Dexamethasone total 1 – 2 days - ICS controller therapy
- LTRA (if indicated)
Asthma action plan (AAP)
Recommended for all children with asthma, especially those with partly or uncontrolled asthma, history of severe exacerbation, & high-risk asthma patients.
Information to be included in the AAP :
- Controlled therapy (doses & frequency)
- List of danger signs, & when and how to seek urgent medical help
- Outline for the patients &/or their carer to recognize symptoms & signs of asthma exacerbation
- Instruction on steps to be taken in response to asthma exacerbation.
Malay version
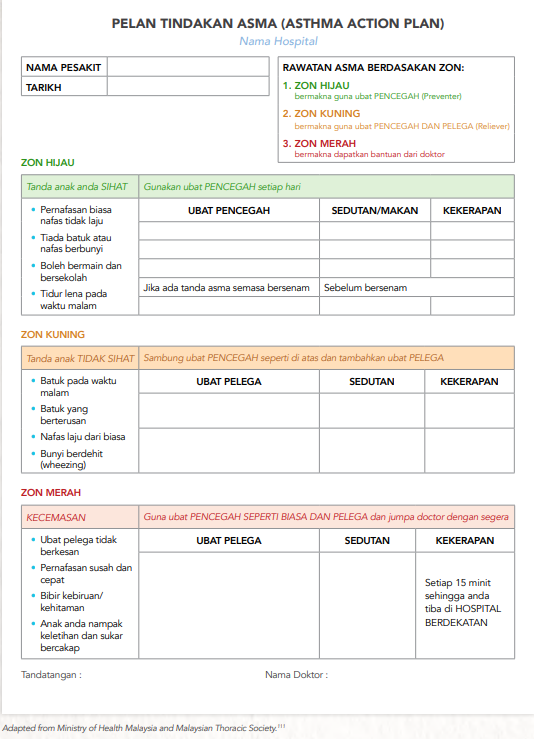
Source: Clinical Practice Guidelines Management of Childhood Asthma 2024 Consensus Statement 4th Edition.
English version
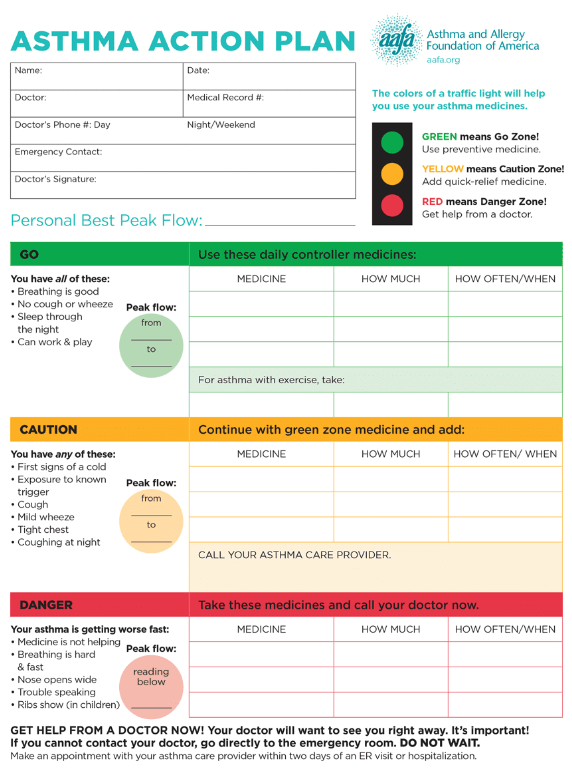
Source: Asthma and Allergy Foundation of America (aafa.org)
Quick guide on initial home management (GINA 2026)
Ideally, patient should follow the written asthma action plan that has been given to them.
In the event that AAP is not available, this quick guide can be used for initial home management.
Step 1 : Give SABA
- 2 puffs of inhaled SABA (100 mcg salbutamol [albuterol] per puff or equivalent), 1 puff at a time via spacer device with or without facemask.
- May be repeated another 2 times at 20 mins interval if needed.
Step 2 : Reassess after 1 hour (or earlier)
Seek immediate attention if :
🚨 Child is acutely distressed.
🚨 Symptoms not relieved promptly by bronchodilator
🚨 The period of relief after doses of SABA is < 4 hours & becomes progressively shorter.
🚨 Child <1 year needing repeated SABA over several hours.
Seek same day review if :
⚠️ ≥ 4 puffs SABA needed for symptoms relief within first 4 hours, OR
⚠️ SABA is needed on > 3 occasions within the first 12 hours.
References
- Malaysian Thoracic Society, Academy of Medicine of Malaysia, & Lung Foundation of Malaysia. (2014). Clinical practice guidelines: Management of childhood asthma.
- Global Initiative for Asthma. (2024). Global strategy for asthma management and prevention (2024 update)
- Global Initiative for Asthma. (2026). Global strategy for asthma management and prevention (2026 update)