Molluscum contagiosum

Molluscum Contagiosum
General features
Causative agent: Molluscum Contagiosum Virus (MCV) – double stranded DNA of the Poxviridae family.
Routes of transmission:
- Direct skin-to-skin contact (including sexual activity)
- Indirectly via fomites (e.g. towels, clothing, gym equipment, toys, swimming pool surfaces & sports gear)
- Autoinoculation – transfer of virus to nearby or distant skin areas by scratching/touching existing lesions.
Incubation period: 2 – 6 weeks
Epidemiology
Most common in children aged 1 – 14 years (US data), especially < 8 years (median diagnosis age ≈ 5 year old). Rare in infants under 1 year of age.
Higher prevalence in warm climates.
In adolescents & adults, transmission often occur via sexual contact or close skin-to-skin contact during sports e.g. wrestling or gymnastics
Also seen more commonly in immunosuppressed individuals who are immunosuppressed (HIV, post-transplant, chemotherapy, primary immunodeficiency) & tend to present with lesions which are:
- More numerous
- Larger (may exceed 10 – 15 mm in diameter “giant” molluscum)
- Atypical in distribution (face, eyelids & mucous membranes)
- Often long-lasting
Children with atopic dermatitis are at increased risk (frequent scratching –> disruption of skin barrier –> facilitating viral entry & autoinoculation).
Pathophysiology
Entry and Replication:
- Virus gains access into the epidermis through microabrasion or a compromised skin barrier.
- Replicates locally within the cytoplasm of keratinocytes, leading to proliferation and formation of typical molluscum lesions.
Immune evasion: Produces proteins that inhibit chemokine signaling and suppress local inflammatory pathways, leading to persistence of lesions for months to years.
MCV infections remain localized to the skin & do not cause viremia or systemic illness.
Clinical features
Often asymptomatic, but can have mild pruritus or local irritation.
Characteristic lesion: flesh-colored, dome-shaped papules with central umbilication, usually 2 – 5 mm in diameter.
Lesions may be solitary or clustered.
Common sites:
- Trunk, extremities & face in children.
- Genital, perineal & lower abdominal areas in sexually active adolescents & adults.

Flesh-colored, dome-shaped papules with central umbilication
Occasionally, they can present as molluscum dermatitis.
Molluscum dermatitis
- An immune-mediated hypersensitivity reaction to MCV antigens, not due to direct viral spread to adjacent skin.
- Appears as erythematous, scaly, or excoriated patches surrounding molluscum lesions.

As the lesion is resolving, it often appears inflamed, red and crusty which is also known as the BOTE (“Beginning Of The End”) sign. It signifies that the immune system is clearing the virus.

Investigation
Molluscum contagiosum is a clinical diagnosis which can be supported by dermatoscopic examination.
Further testing (e.g. lab test, skin biopsy & FNAC) is considered when:
- Lesion has atypical morphology or unusual distribution.
- The patient is immunocompromised, or
- When the diagnosis is uncertain.
True bacterial superinfection of MC lesions is uncommon, thus routine culturing or antibiotic use is not recommended.
Management
Observation (“benign neglect”) has been the 1st line approach in immunocompetent individuals, given the lack of consistently superior interventions & self-limited nature of the infection (as most cases resolve spontaneously within months to years).
- Spontaneous resolution is expected in most cases within 6 – 18 months, occasionally up to 2 – 3 years.
- Recurrent is uncommon, but reinfection can occur with new exposure.
Treatment is often considered for persistent, symptomatic, or cosmetically concerning lesions or to reduce transmission risk.
However, the management of molluscum contagiosum is increasingly moving toward active treatment, driven by recognition of its adverse consequences and the development of FDA-approved topical therapies.
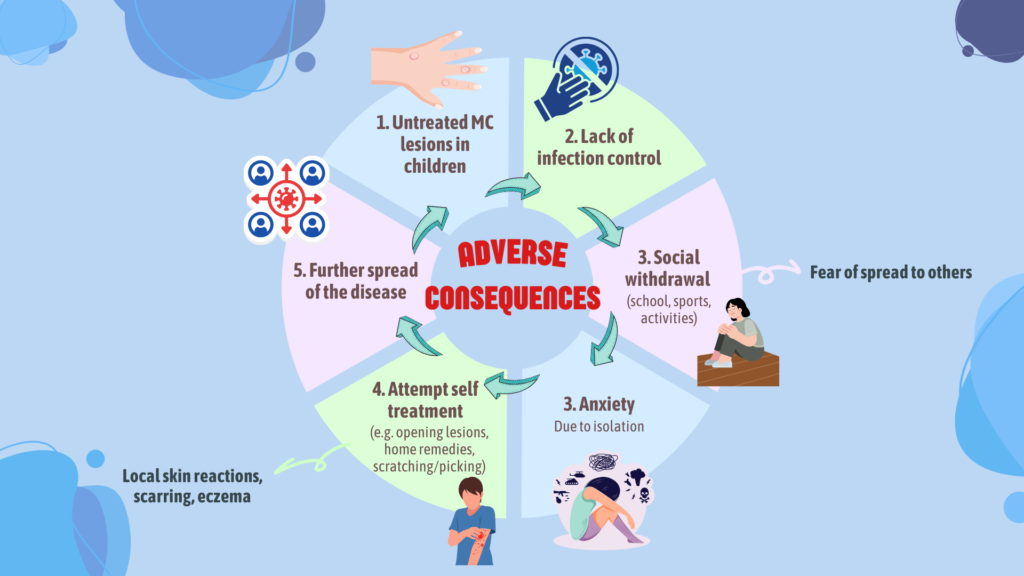
Cycles of adverse consequences related to untreated molluscum contagiosum
Treatment options
Should be based on lesion burden, symptoms, patient preference & risk of transmission.
Can be physical method or topical therapies.
Clinician applied (In-clinic)
Physical method:
- Curettage – often the most effective; high clearance and good cosmetic outcomes; commonly preferred in children.
- Cryotherapy – may be painful; risk of blistering and pigmentary changes.
- Electrodessication – less preferred due to higher residual lesions and slower recovery
Topical therapy:
- Cantharidin 0.7% (VP-102) – FDA-approved formulation applied in clinic using a single-use applicator.
Patient applied (At-home) – topical therapy
FDA-approved:
- Berdazimer gel (Zelsuvmi) – approved for adults and children ≥1 year; once-daily topical application by patients, parents, or caregivers.
Off-label options:
- Potassium hydroxide
- Benzoyl peroxide
- Salicylic acid
- Podphyllotoxin
Interestingly, oral cimetidine may also have a role in MC management and may be beneficial in those with atopic dermatitis or having lesions covering most of the body.
Not recommended
Imiquimod (topical immune response modifier) – not recommended due to its lack of effectiveness & increased risk of local application-site reactions.
Differential diagnosis
1. Verruca vulgaris (common warts)
- Caused by HPV.
- Presents as flesh-colored, hyperkeratotic papules usually on the hands & feet. They typically have a rough surface & lack central umbilication
2. Verruca plana (flat warts)
- Also HPV-related.
- Appear as small, flat-topped papule on the face & extremities, especially in children & young adults. They are less dome-shaped than molluscum & also lack central umbilication.
3. Condyloma acuminatim – anogenital warts caused by HPV types 6 & 11.
References
- Hebert, A. A., Bhatia, N., & Del Rosso, J. Q. (2023). Molluscum Contagiosum: Epidemiology, Considerations, Treatment Options, and Therapeutic Gaps. The Journal of clinical and aesthetic dermatology, 16(8 Suppl 1), S4–S11.
- Bhatia, N., Hebert, A. A., & Del Rosso, J. Q. (2023). Comprehensive Management of Molluscum Contagiosum: Assessment of Clinical Associations, Comorbidities, and Management Principles. The Journal of clinical and aesthetic dermatology, 16(8 Suppl 1), S12–S17.
- Kumar G, Stern J, Daley SF. Molluscum Contagiosum. [Updated 2025 Dec 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441898/