Constipation in children

Constipation (Functional) in Children
2 subtypes
- Organic 5% (structural, neurologic, toxic/metabolic/GI disorder)
- Functional 95%, most common among paediatric population.
We will be focusing mostly on functional constipation as this is most frequently encountered & managed in primary care settings.
Pathophysiology of constipation
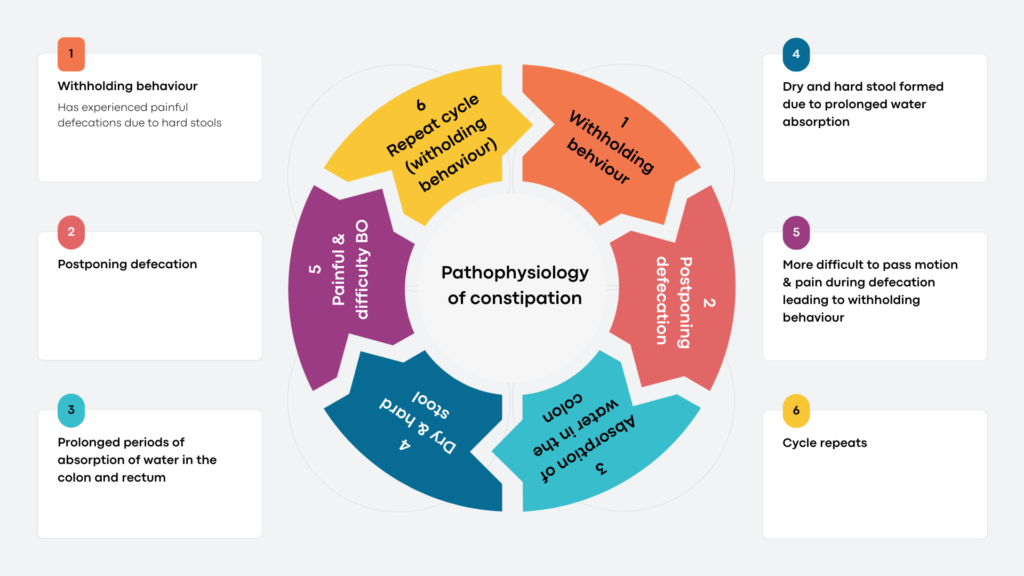
Repeated cycles lead to fecal impaction and may cause overflow incontinence.
Prolonged periods of withholding and fecal impaction eventually may cause increased in rectal compliance –> Larger volume of stools required to generate an urge for defecation –> increased stool retention.
It is important to keep in mind that psychological factors may also have a role, e.g. stress, adverse life events, bullying, anxiety, physical/sexual abuse.
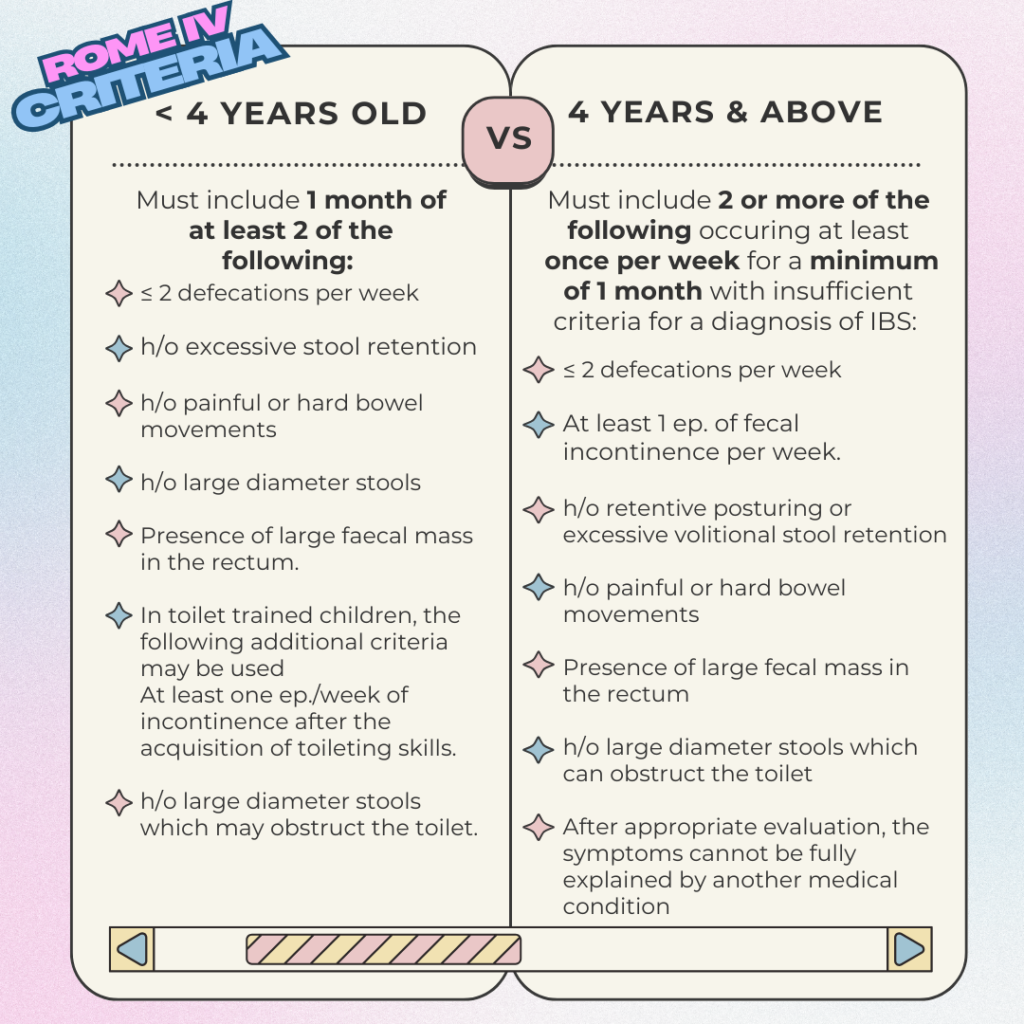
Diagnostic Criteria (Rome IV)
Differential diagnosis of functional constipation (FC)
Mainly the organic causes of constipation:
- Allergy – cow’s milk protein intolerance &/or other food protein intolerance
- Coeliac disease
- Hypothyroidism
- Cystic fibrosis
- Electrolyte abnormalities – hypercalcemia, hyperkalemia
- Drugs – opiates, phenobarbital, anticholinergics
- Neuropathic disorders – Hirschsprung’s disease, Internal sphincter achalasia
- Spinal cord abnormalities – myelomeningocele, tethered spinal cord, syringomyelia
- Anatomic malformations – imperforate anus, anteriorly displaced anus
- Psychososial – depression/anxiety, sexual abuse, toilet training
Red Flags to look out for 🚨
| Red Flags | Disorders |
|---|---|
| Failure to pass meconium < 48 hours after birth | Hirschsprung’s |
| Onset of constipation – from birth or 1st week of life | Congenital, mechanical obstruction |
| Stool consistency – ribbon/pencil-thin stools | Anorectal malformation |
| Bloody diarrhea | Infection, inflammatory bowel disease, cow’s mild protein allergy |
| Developmental delay | Metabolic or other |
| Lower limb neurology or urinary incontinence in older child | Spinal pathology |
| Other physical signs: lethargy, fever, bilious vomiting, rash | Infection, obstruction, metabolic |
Assessment
Establish diagnosis of functional constipation by asking about the bowel habit in accordance to the ROME IV criteria.
Enquire about withholding behaviour which may include:
- Going stiff
- Clenching buttocks
- Walking on tip toes
- Crossing legs
- Bracing against furniture
- Being in all fours position or curling up in a ball
- Sitting with legs straight out

Associated symptoms of constipation
It is important to assess also for the associated symptoms which may include:
- Change in appetite
- Faecal soiling
- Nausea/vomiting
- Weight loss
- Recurrent UTI
- Daytime urinary incontinence
- Perianal fissure/dermatitis/fistula/abscess
Investigations are usually only indicated when an organic cause is suspected or if the child does not respond to treatment despite optimal treatment.
Non-pharmacological management

- Dietary modification
– Do not use dietary interventions alone as first-line treatment for idiopathic constipation.
– Infants are encouraged to continue breastfeeding.
– Juices containing sorbitol (e.g. apple, prune, pear) can help to increase stool water content and stool frequency.
– Recommended amount of prune juice for infant < 6 months: 1 – 3 mL/kg diluted with 30 – 60 mL of water.
– Achieving the daily fiber and fluid requirement intake (exceeding the daily requirement does not improve constipation in children)
– The recommended daily fluid intake is approximately 4 cups per day for children one to three years of age, 5 cups for children four to eight years of age, and 7 to 8 cups for older children. Children and adolescents obtain adequate daily fiber intake from five servings of fruits and vegetables. Recommended daily fiber intake can be calculated by adding 5 g to the child’s age in years. https://www.aafp.org/pubs/afp/issues/2022/0500/p469.html#afp20220500p469-sort6 - Education – about the pathophysiology of FC, accompanying fecal incontinence and important of treatment adherence.
- Toilet training is added to the treatment for children with a developmental age of at least 4 years.
- Enhancing self-efficacy (the belief that one has the skill to succeed at a goal, and treatment success) in the child may improve treatment outcome.
Pharmacological management 💊
(3 phases – Disimpaction, Maintenance, Weaning)
1. Disimpaction
Improves the response to maintenance treatment.
Signs of impacted stool: overflow incontinence, palpable faecal mass over the abdomen.
1st line: Polyethylene glycol (PEG) [enemas can be prescribed if PEG not available]. Alternatively, lactulose can be used if PEG is not available (both PEG and lactulose can achieve disimpaction, though PEG’s effect is significantly faster). Other oral pharmacological agents can also be considered for disimpaction if PEG & enemas are not tolerated/ineffective
2. Maintenance
1st choice: PEG
Alternative: Lactulose (if PEG is not available)
ESPGHAN/NASPGHAN guidelines: TCA 2 weeks to assess effect and intensify accordingly. Treatment should be continued for at least 2 months.
3. Weaning
After 2 months of treatment, weaning can be initiated when symptoms are sufficiently reduced or absent for at least 1 month (Does not fulfill Rome IV criteria anymore)
Dosages & frequency should be reduced gradually in order to prevent relapse.
General guidelines regarding pharmacological management
Oral laxatives usually work.
May consider osmotic + stimulant laxatives combination in older children.
Enema has faster effect but may be challenging or traumatising.
Some common pitfalls in management:
- Initiation of maintenance therapy before dis-impaction in children with impacted stool.
- Dis-impact without maintenance therapy
- Giving too low a laxative dose
- Stopping laxatives too soon.
About pharmacological agents
Osmotic laxatives
1st choice for maintenance treatment.
Poorly absorbed in the gut –> increased in osmolarity –> water influx into intestinal lumen –> stool softening.
a. Polyethylene glycol (PEG)
- PEG is generally considered 1st line for both disimpaction & maintenance.
- Administered orally with or without electrolytes (addition of electrolytes may deteriorate the palatability of PEG).
- Available as PEG 3350 and PEG 4000 (the numbers represent the molecular weight e.g. 3.350 and 4.000 g/mol respectively)
- Advised dosage:
– For disimpaction – 1 – 1.5 g/kg/day for 3 days (maximum 6 consecutive days)
– For maintenance – 0.2 – 0.8 g/kg day (suggested starting dose of 0.4 g/kg/day); can be administered OD or divided in several doses. - Side effects: Diarrhea, bloating, flatulence, nausea, vomiting, abdominal cramps
- In patients with water & electrolyte disturbances, monitoring of serum electrolytes should be done and PEG with electrolytes should be prescribed with caution.
b. Lactulose
- Fermented into low molecular weight acids in the colon by bacterial enzymes –> osmotic effect & reduce fecal pH (stimulates colonic peristalsis)
- Has more evidence available on the efficacy of lactulose usage during maintenance than mineral oil & magnesium hydroxide.
- Lactulose is safe for all ages.
- Side effects: abdominal gas, bloating, cramping
- Advised dosage: 1 ml/kg once or twice daily
- Alternatively:
– Adults – 15ml, taken twice a day as a starting dose
– Children aged 5 to 17 years – 5ml to 20ml, taken twice a day
– Children aged 1 to 4 years – 2.5ml to 10ml, taken twice a day
– Babies aged 1 month to 11 months – 2.5ml, taken twice a day
c. Magnesium hydroxide (also known as milk of magnesium)
- Hyperosmolar agent. Hypothesis that magnesium may help with constipation comes from study showing that infants receiving magnesium-rich formula were reportedly to have a significantly softer stool consistency & higher defecation frequency.
- Associated with poor palatability.
- Side effects: diarrhea, abdominal pain, bloating.
- Should be used with caution in those with impaired renal function due to increased risk of hypermagnesemia.
- Oral magnesium citrate is predominantly used for bowel cleansing prior to colonoscopy in children & there is little evidence for the use in treatment of FC in children.

Enemas
Predominantly used for disimpaction. Should not be used for maintenance treatment.
Types:
- Sodium docusate (stimulates retention of water in stools)
- Sodium lauryl sulfoacetate (redistribute water that is bound to hard feces –> soften feces) – predominantly prescribed in infants.
- Sodium phosphate (hyperosmolar phosphate solution) – contraindicated in Hirschsprung’s disease or renal insufficiency.
- Glycerine
- Bisacodyl
Common adverse events: abdominal pain, emesis, diarrhea
Adverse events are generally minor and low rate.
Stimulant laxatives
Additional or 2nd line treatment of FC in children when osmotic laxatives alone are not sufficient.
MOA: Stimulation of enteric nervous system –> enhance peristalsis.
Generally well tolerated, common side effect include abdominal pain.
Types:
- Diphenylmethane (e.g. bisacodyl & sodium picosulfate)
- Anthraquinones (e.g. senna)
a. Diphenylmethane – bisacodyl & sodium picosulfate
Bisacodyl
- Can be given orally or rectally.
- Oral: 5mg OD (for children >= 3 years old)
- Rectal: 5 mg OD (for >= 2 years old) – contraindicated in patients with proctitis or anal fissures.
- Promising results for effectiveness & long term were reported by a retrospective stud in 164 children with FC refractory to conventional treatment.
Sodium picosulfate
- Can only be administered orally.
- Studies lacking.
Common side effects of both: abdominal pain, nausea & diarrhea
b. Anthraquinones – Senna
- Can only be administered orally.
- Little evidence available regarding its efficacy.
- Common side effects: diarrhea, abdominal pain, nausea, & flatulence.
- Young children are at risk of diaper rash, blisters & peeling skin.
Lubricants – mineral oil (liquid paraffin)
MOA: softening/lubricating stools.
Orally administered, not absorbed by colon or small bowel.
Considered to be safe for treatment of FC in children.
Side effects:
- Most common: abdominal pain, nausea, vomiting, diarrhea & flatulence.
- Leakage out of the anus –> irritated skin around the anus & clothes staining.
- Severe A/E: granulomas of the intestinal tract, lipoid pneumonia
Contraindications:
- < 3 years old
- Swallowing difficulties (risk of lipoid pneumonia)
- Coagulation disorders (theoretical risk of reducing absorption of fat-soluble vitamins.
References
- Singh, H., & Connor, F. (2018). Paediatric constipation: An approach and evidence-based treatment regimen. Australian journal of general practice, 47(5), 273–277. https://doi.org/10.31128/AFP-06-17-4246
- Mulhem, E., Khondoker, F., & Kandiah, S. (2022). Constipation in Children and Adolescents: Evaluation and Treatment. American family physician, 105(5), 469–478.
- de Geus, A., Koppen, I. J. N., Flint, R. B., Benninga, M. A., & Tabbers, M. M. (2023). An Update of Pharmacological Management in Children with Functional Constipation. Paediatric drugs, 25(3), 343–358. https://doi.org/10.1007/s40272-023-00563-0