UTI in pregnancy

Urinary Tract Infection in Pregnancy
Asymptomatic Bacteriuria (ABU)
Definition: Bacterial monoculture ≥ 10⁵ CFU/ml in a single urine culture taken in women without UTI symptoms.
ABU in pregnancy should be treated.
Untreated ABU in pregnancy can lead to increased risk of symptomatic cystitis & acute pyelonephritis.
Acute pyelonephritis in pregnancy is associated with adverse perinatal outcome including risk of premature delivery &/or low birth weight.
Common organisms involved:
- Escherichia coli (63 – 85%)
- Klebsiella pneumoniae (~8%)
- Coagulase-negative Staphylococcus (up to 15%)
- Staph aureus (up to 8%)
- Group B Streptococci (GBS) (2 – 7%)
The ACOG recommends screening for ABU at the first prenatal visit, whereas the RCOG recommends routine midstream urine screening for ABU in early pregnancy.
However, our Malaysia consensus guidelines on the management of UTI in pregnancy do not recommend routine screening for ASB in pregnancy, though it may be considered in those with high risks.
These risks include:
- Diabetes mellitus
- Underlying renal tract abnormalities
- Past or recent renal calculi
- Recurrent infection
- Young
- Less educated
- Nulliparous
- Late antenatal care booking
- Active smoking during pregnancy
Our NAG guideline on the other hand recommends investigating for ABU if proteinuria is detected on routine albumin/sugar screening.
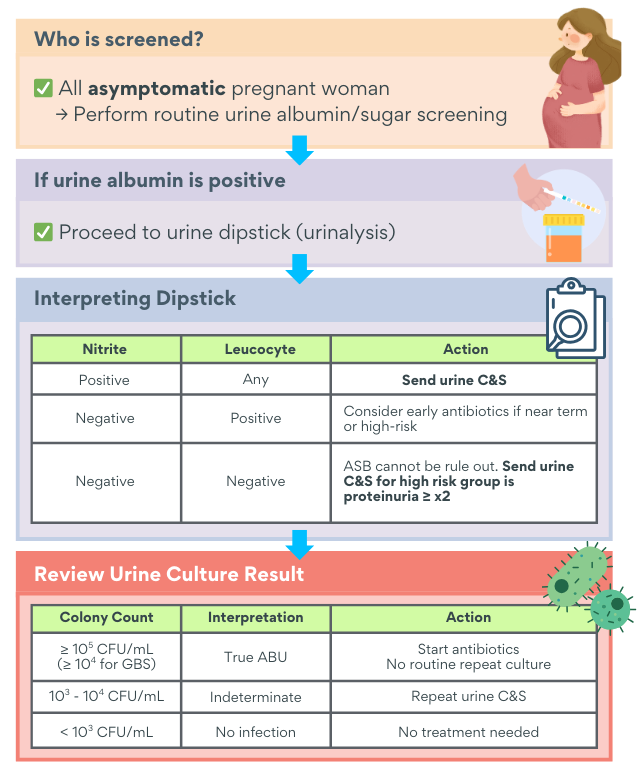
Diagnosis of ABU
Midstream urine culture is the gold standard.
Positive: Bacterial monoculture ≥ 10⁵ CFU/mL
For group B streptococcus: CFU of 104 is used as the threshold for treatment as it is indicative of vaginal colonization – to prevent GBS in infant
For borderline bacteriuria (CFU/ml of 103 – 104) or polybacterial culture: Repeat test after 1 week
Management of ABU in pregnancy
The presence of ABU in pregnancy women is an absolute indication for initiation of treatment.
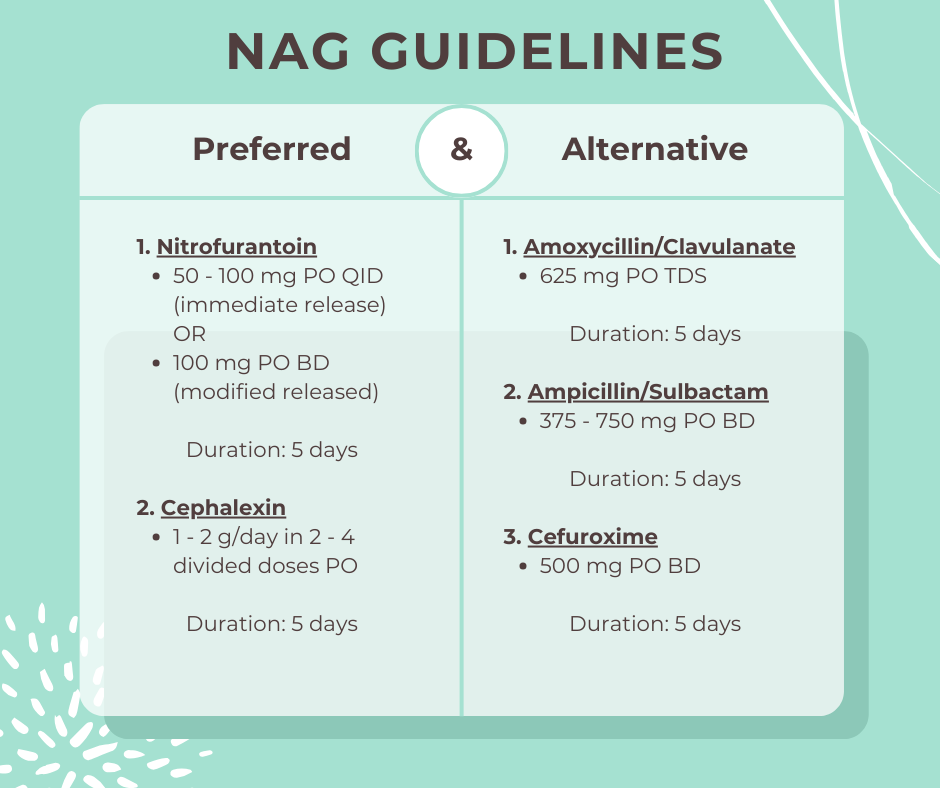
Further comments
- Nitrofurantoin is contraindicated if eGFR < 30 mL/min & should be avoided in 1st and 3rd trimester.
- Amoxycillin/Clavulanate is generally safe in pregnancy (Category B) except for an increasing incidence of necrotizing enterocolitis in preterm babies & in babies born after premature rupture of membrane.
- Repeat urine culture after treatment is not routinely recommended.
Lower Urinary Tract Infection (LUTI) – Acute cystitis, urethritis
Symptoms:
- Dysuria
- Cloudy urine
- Hematuria
- Abdominal or suprapubic discomfort/pain
- Urgency & frequency.
Patients are usually afebrile & have no evidence of systemic illness.
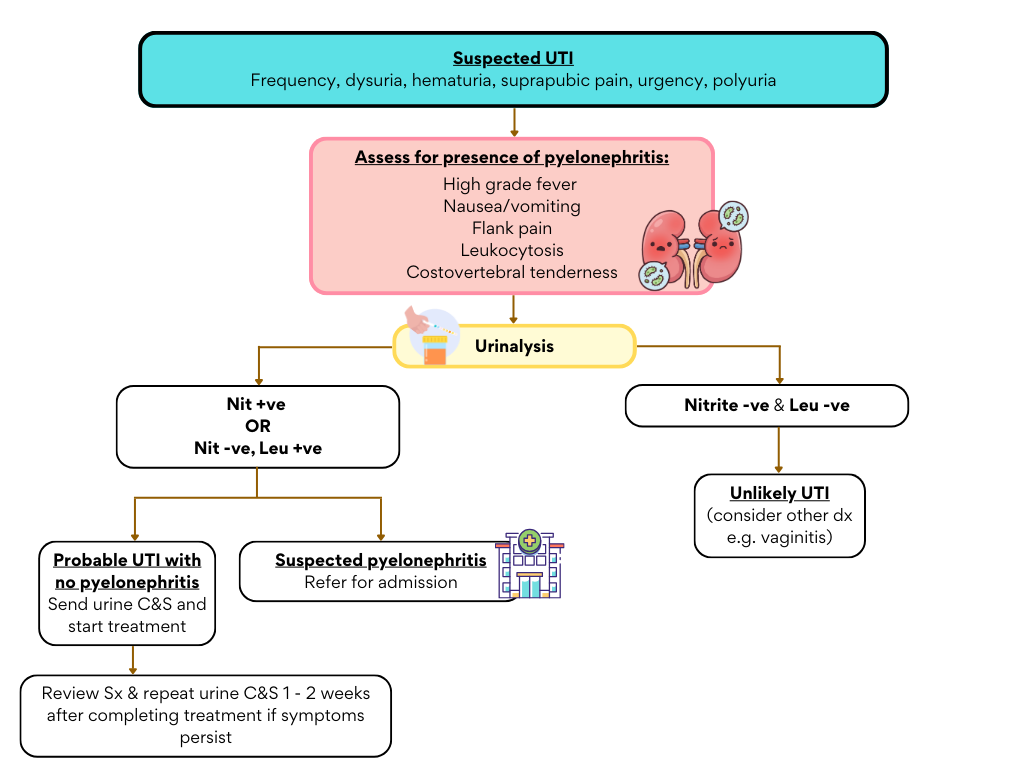
UTI should be suspected based on symptoms, supported by positive urinalysis and confirmed by urine culture.
- UTI can be excluded if the urine dipstick is entirely normal (ACOG guideline)
- The diagnosis is confirmed by presence of even small bacterial colony counts (≥ 102 – 103 CFU/ml).
Management of LUTI in pregnancy
Treatment is initiated before culture results are available.
Under-treatment can lead to persistent infection & risk of progression to pyelonephritis
Antibiotic of choice to start is as above in ABU section with the same dosage and frequency. The minor difference would be the duration of treatment which is 5 – 7 days.
Repeat urine culture may be considered 1 – 2 weeks after completing treatment or repeat only if symptoms recur (ACOG guideline)
Acute pyelonephritis
Most common in late pregnancy & is usually due to undiagnosed or inappropriately treated LUTI, or untreated ABU.
All pregnancy associated pyelonephritis = complicated nephritis
Complications of acute pyelonephritis may include:
- Perinatal – Preterm labor, Low birth weight
- Mother – AKI, preeclampsia, urosepsis, septic shock, ARDS
Pyelonephritis is suggested clinically by symptoms of:
- Flank or renal angle pain, costo-vertebral tenderness or pyuria.
- Fever &/or other systemic features like rigor, nausea & vomiting.
Diagnosis can be made by combination of symptoms, FBC, inflammatory markers, RP, blood culture, urine C&S (the presence of even small bacterial colony counts: ≥ 102 – 103 CFU/ml).
Acute pyelonephritis should prompt an urgent referral to tertiary care for admission and management with IV antibiotics.
Algorithm for suspected UTI in pregnancy
References
- Ministry of Health Malaysia. (2021). Consensus guidelines on the management of urinary tract infection in pregnancy. Family Health Development Division.
- Ministry of Health Malaysia. (2025). Urinary tract infection in pregnancy (asymptomatic bacteriuria). National Antibiotic Guideline (NAG).
- Ministry of Health Malaysia. (2025). Urinary tract infection in pregnancy (symptomatic). National Antibiotic Guideline (NAG).
- American College of Obstetricians and Gynecologists. (2023). Urinary Tract Infections in Pregnant Individuals. Obstetrics & Gynecology, 142(2), 435–445. doi.org.