Urinary Tract Infection (UTI)
Urinary Tract Infection (UTI)
Definition
- Asymptomatic bacteriuria: Urine bacterial growth ≥ 105 cfu/mL in 2 serial samples in women or a single sample in man without UTI symptoms
- Uncomplicated UTI: Acute, sporadic or recurrent lower (uncomplicated cystitis) &/or upper (uncomplicated pyelonephritis) UTI, limited to non-pregnant women with no known relevant anatomical & functional abnormalities within the urinary tract or comorbidities
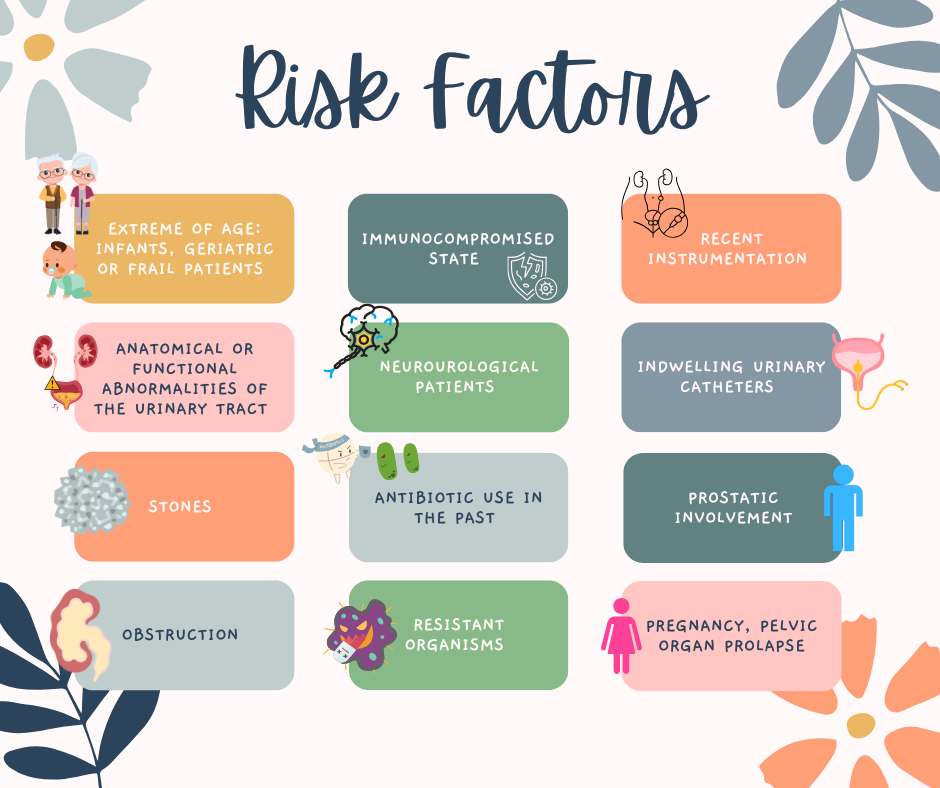
- Complicated UTI – UTI with increased risk of a complicated course:
- All men
- Pregnant women
- Anatomical or functional abnormalities of the urinary tract
- Indwelling urinary catheters
- Renal diseases
- Concomitant immunocompromising diseases (e.g. uncontrolled DM)
- Catheter-associated UTI (CAUTIs): UTI in a person who is currently catheterized or has had a catheter in place within the past 48 hours.
- Urosepsis: Sepsis secondary to infection originating from the urinary tract
- Recurrent UTI: Recurrence of uncomplicated &/or complicated UTIs, at least 3 ep./year or 2 UTIs in the last 6 months.
- Upper UTI: Involves the ureters (ureteritis) and kidneys (pyelonephritis)
- Lower UTI: Infection of the bladder (cystitis)
Asymptomatic bacteriuria (ABU)
Men & non-pregnant women with asymptomatic bacteriuria should not be started on antibiotics.
Antibiotics should only be prescribed for ABU in 2 conditions:
- Pregnancy
- Prior to urological procedures where there is possibility of mucosal breaching
This is consistent with the EAU guidelines.
Do not screen or treat ABU in the following conditions:
- Women without risk factors
- Post-menopausal women
- Patients with indwelling or suprapubic catheters & nephrostomy tube
- Elderly institutionalized patients
- Patients with dysfunctional &/or reconstructed lower urinary tracts
- Patients with renal transplants
- Patients prior to arthroplasty surgeries
- Patients with h/o recurrent UTI
Common organisms involved
- Escherichia coli
- Klebsiella pneumoniae
- Streptococcus agalactiae (Group B streptococcus) – significant to treat in pregnant women
- Coagulase-negative staphylococcus
- S. aureus
UTI risk factors
General UTI symptoms
- Dysuria (pain, burning, stinging)
- Urgency
- Frequency
- Incontinence
- Urethral purulence
- Pressure or cramping in the lower abdomen
- ± Systemic SSx of infection: Fever, Sepsis features (in urosepsis), etc.
The UK guideline has indicated there are 3 key urinary symptoms (for women under 65 years): Dysuria, New nocturia and cloudy urine.
- If 2 out of 3 symptoms are positive – UTI is likely & dipstick is not needed.
- If only 1 symptom positive – Proceed with urine dipstick for further assessment.
Warning signs that require further assessment & management include: pyelonephritis (flank pain, fever with chills and rigors, nausea or vomiting), sepsis, cancer.
It is important to rule out genitourinary causes of urinary symptoms in women.
- Vaginal infection: Enquire regarding vaginal discharge or vaginal irritation
- Urethritis (post sexual intercourse, irritants, or sexually transmitted infection). It is important to rule out sexual transmitted diseases (by assessing for any high risk behavior), if not opportunities might be missed to diagnose & treat STI. [This point applies to both male & female patients]
- Genitourinary symptoms of menopause/atrophic vaginitis/vaginal atrophy.
Approach in adults > 65 years with suspected UTI (UK guideline).
It is important to note that the approach differ slightly in adults > 65 years.
Urine dipstick is not recommended as it is less reliable.
- Asymptomatic bacteriuria is commonly seen in older adults and can cause a positive urine dipstick, though often time it is not harmful. Starting antibiotics based on this are not beneficial & may cause harm.
The diagnosis of UTI instead relies more on symptoms/signs alone.
- First: Rule out sepsis/pyelonephritis
- Next: Check for any NEW symptoms/signs of UTI
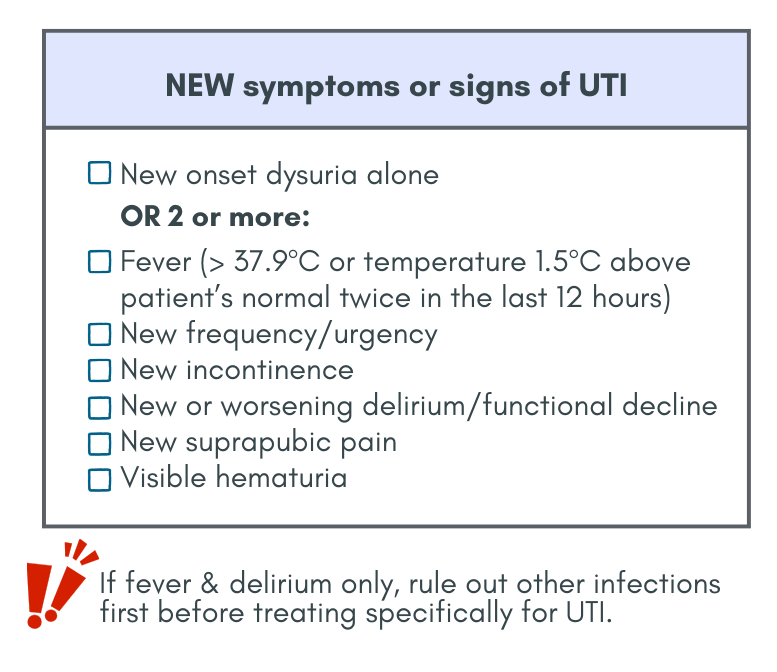
If the criteria are fulfilled, then UTI is LIKELY.
Management:
- Send for urine culture before starting antibiotics.
- If mild symptoms in women without catheter & low risk of complications, consider delayed antibiotic prescription. However, if more severe symptoms or high risk of complications, start antibiotics promptly
- For men, initiate antibiotics immediately.
Approach to suspected UTI in Adults, Non-pregnant
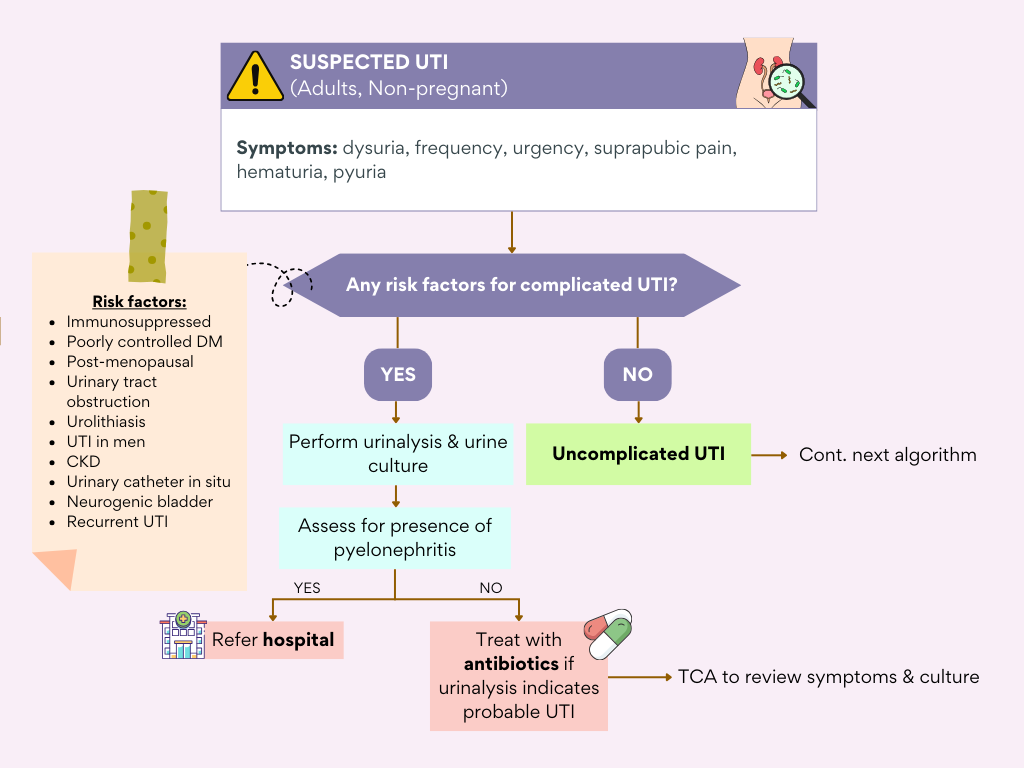
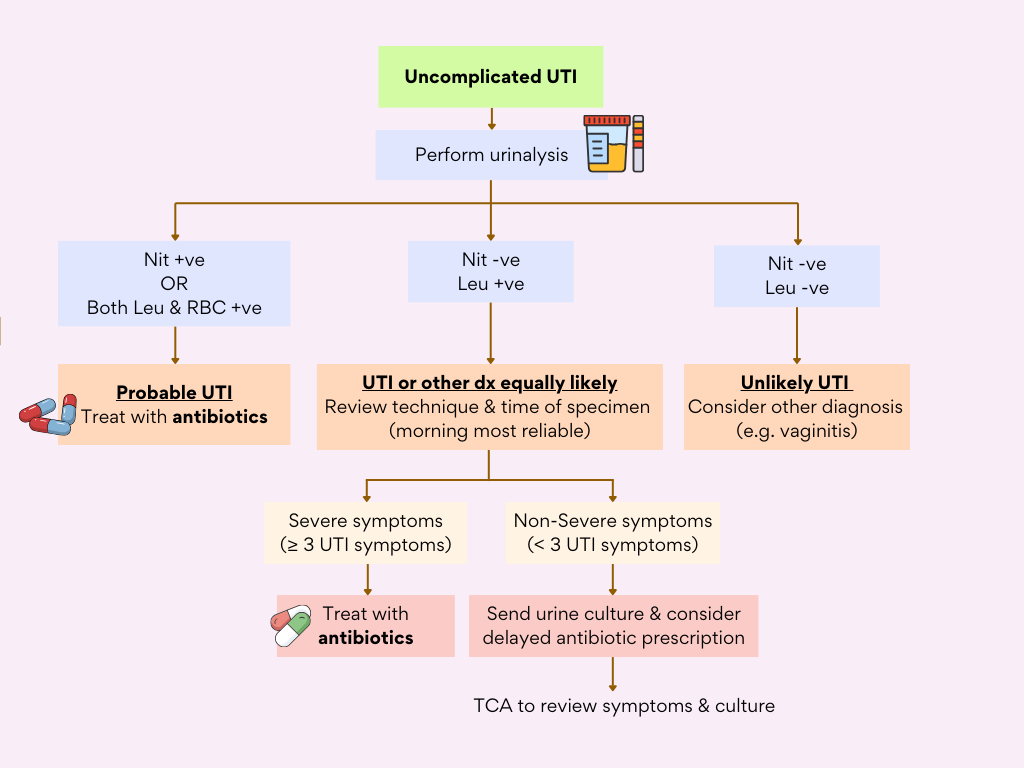
Severe symptoms (patient has ≥ 3 symptoms suggestive of UTI). These symptoms include dysuria, urgency, frequency, loin pain/suprapubic pain, polyuria, worsening incontinence & hematuria.
This algorithm has also provided a guide to approach urinalysis with either nitrite or leucocyte positive which is often encountered in daily clinical practice.
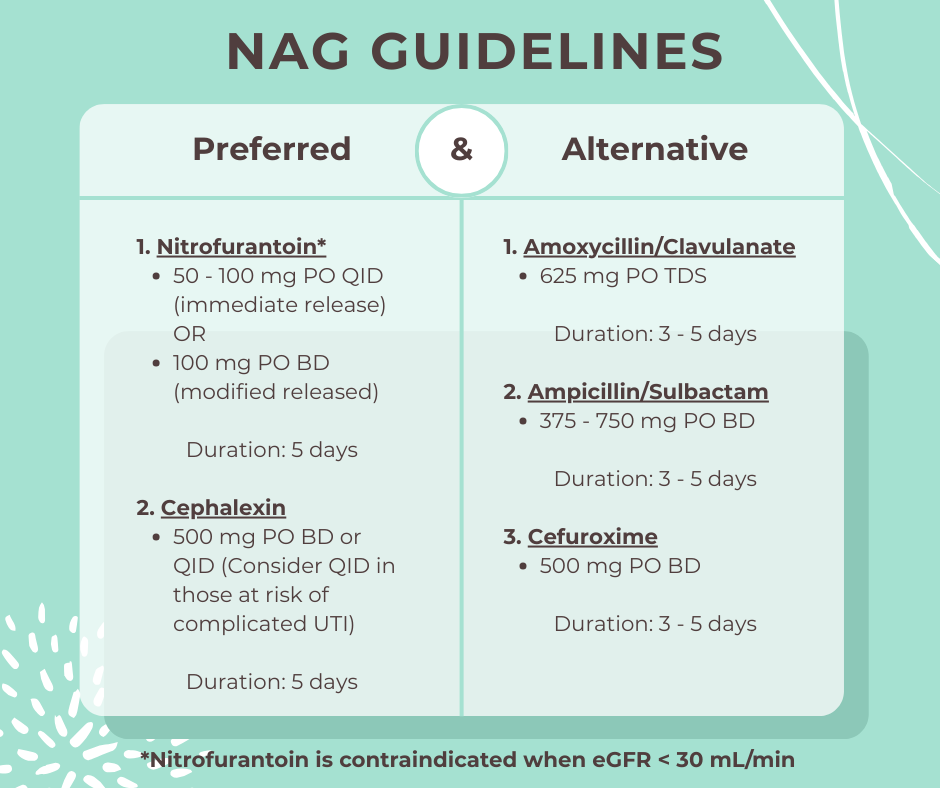
Management
Further comments
Ciprofloxacin & other fluoroquinolones are highly efficacious in 3-day regimens but have risk of collateral damage, thus should be reserved for:
- Definitive therapy or severe infections
- Those who cannot tolerate the recommended antibiotics either due to adverse effects or allergy
Trimethoprim-sulfamethoxazole is not recommended as empirical therapy due to local resistance rate or E.coli & Klebsiella pneumoniae has been consistently > 30%. If indicated/susceptible, can start 160/800 mg BD for 3 days
Amoxicillin or ampicillin should not be used empirical treatment due to relatively poor efficacy and prevalence of antimicrobial resistance.
NICE guidelines recommendation on duration of antibiotic treatment for UTI :
Non-pregnant women with uncomplicated lower UTI: 3 days
Men and pregnant women with uncomplicated lower UTI: 7 days
Patients started on antibiotic should be reassessed if symptoms worsen rapidly, or shows no improvement within 48 hours of taking the antibiotic.
Regarding Catheter-associated UTI (CA-UTI)
In adults with indwelling urinary catheter, urine dipstick is not reliable to detect UTI as catheters can quickly become colonised with bacteria resulting in a positive dipstick result.
In these group of patients, signs & symptoms are assessed to diagnose UTIs with urine C&S used to support the diagnosis & guide treatment.
Pyuria alone in otherwise asymptomatic patient is not diagnostic of CA-UTI. Whenever indicated, change catheter prior to starting treatment.
For mild or moderate CAUTIs, where patient is stable with no signs of systemic infection, oral antibiotics may be sufficient. The choice between oral & IV antibiotics should be guided by clinical judgement, patient’s overall condition, & results of urine C&S.
References
- Ministry of Health Malaysia. (2024). National antimicrobial guideline (NAG): Urinary tract infection in non-pregnancy (C7). Pharmaceutical Services Programme, Ministry of Health Malaysia.
- Bonkat, G., Kranz, J., Cai, T., Geerlings, S. E., Köves, B., Pilatz, A., Schneidewind, L., Schubert, S., Veeratterapillay, R., & Wagenlehner, F. (2025). EAU guidelines on urological infections. European Association of Urology.
- UK Health Security Agency & NHS England. (2025, July 7). Diagnosis of urinary tract infections: Quick reference tools for primary care. GOV.UK. Retrieved February 19, 2026, from https://www.gov.uk/government/publications/urinary-tract-infection-diagnosis/diagnosis-of-urinary-tract-infections-quick-reference-tools-for-primary-care
- National Institute for Health and Care Excellence. (2019). Urinary tract infection (lower): Antimicrobial prescribing (NICE guideline NG109).