Colorectal cancer screening

Colorectal cancer screening
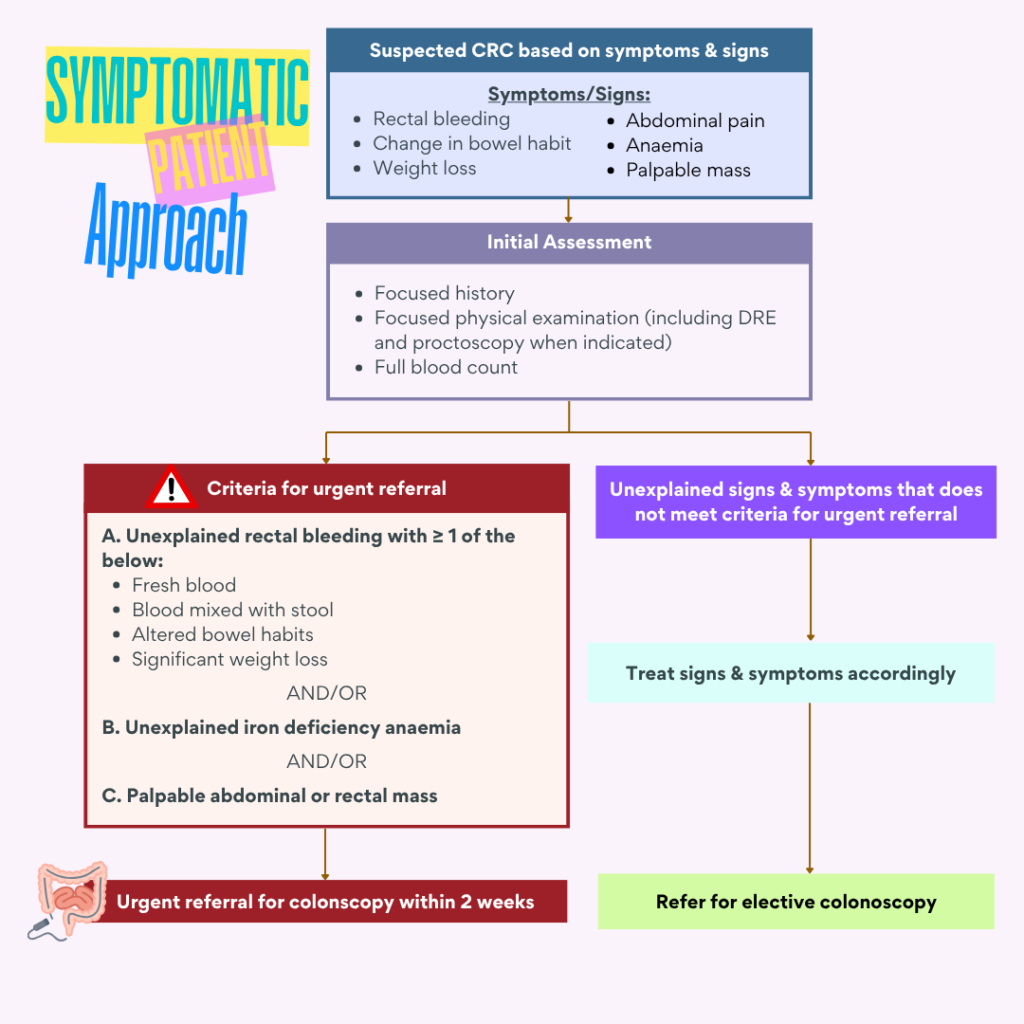
Symptoms of Colorectal Carcinoma (CRC)
Common symptoms
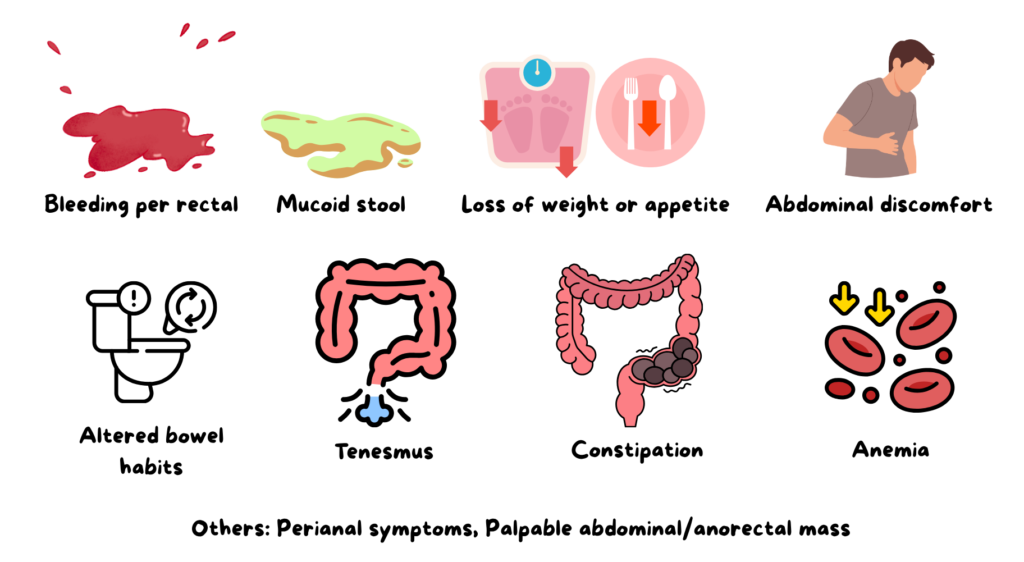
It is important for us to be aware of the various presentation of CRC, so that timely assessment & referral can be done.
Screening modalities
Screening methods for colorectal cancer includes:
1. Fecal test – can detect either the presence of
- Blood (Fecal Occult Blood Test – FOBT) or
- Proteins (e.g. enzyme M2-PK & DNA) – Not widely used due to high cost
2. Flexible sigmoidoscopy
- Advantages: less rigorous bowel preparation, clinic-based, no sedation
- Disadvantages: unable to detect proximal lesions
3. Colonoscopy
- Both diagnostic & therapeutic.
- Able to visualize the colonic mucosa & excise polyps.
4. Colon capsule endoscopy
- Advantage: less invasive
- Disadvantage: unable to perform biopsy or polyps removal
5. Computed Tomographic (CT colonography)
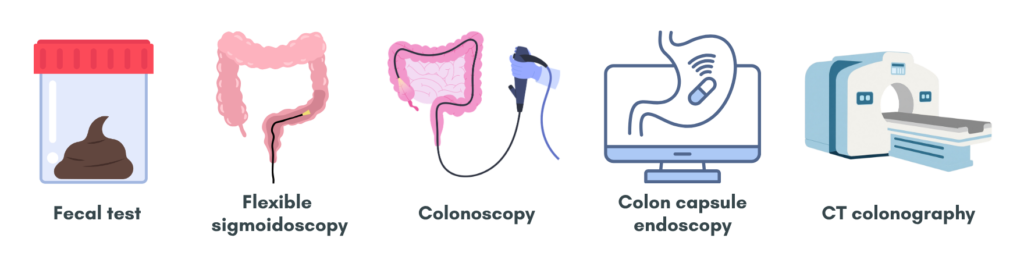
Among these, iFOBT & colonoscopy are the most commonly used.
Fecal test for enzyme M2-PK are available however with a higher cost compared to iFOBT.
Regarding Tumor Markers
- There are no guidelines for using Carcinoembryonic Antigen (CEA) as a screening tool.
- It can be used for monitoring of treatment response but should not be relied as a screening tool.
- A normal CEA does not rule out CRC.
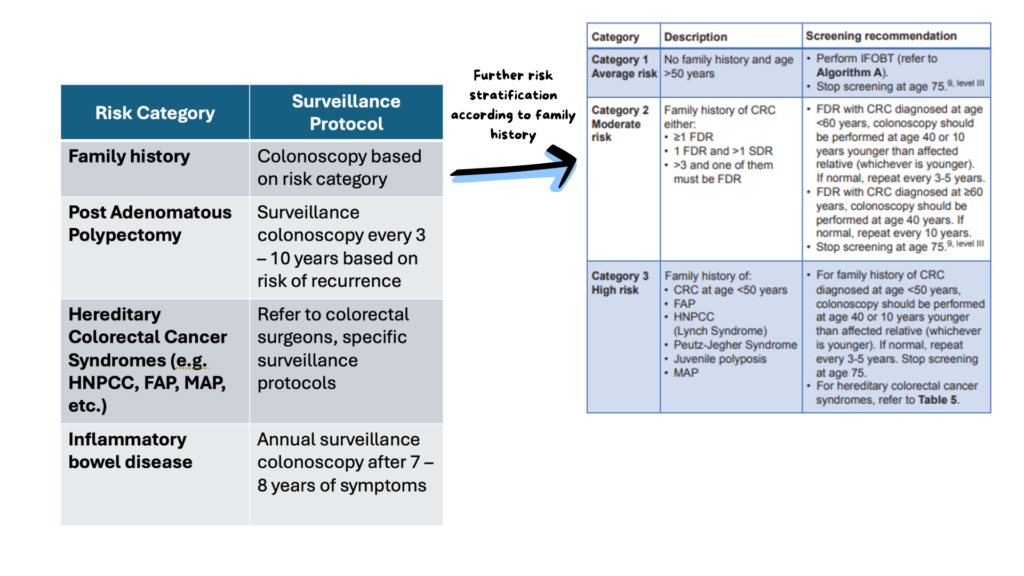
Risk stratification – for Asymptomatic Individuals
Risk stratification will guide the screening modality used, age to start screening & interval of screening.
Individuals can generally be categorized into either:
- Average risk OR
- With risk factors
a) Average risk = population with no known risk for colorectal carcinoma (CRC)
For this group of population, CRC screening is recommended:
- Starting at age 50 (or age 45 per updated USPSTF guidelines)
- Continuing until 75 years of age.
For ages 76 – 85, decision for screening should be individualized based on health, screening history, and patient preference.
In adults aged 86 years and older, evidence for colorectal cancer screening is limited, and competing mortality risks (from other causes) likely outweigh any potential survival benefit.
b) With risk factors (to guide screening)
Other risk factors to consider:
- Smoking
- Diabetes mellitus
- BMI (overweight or obese)
- Alcohol consumption (> 30g/day)
- Processed meat and red meat consumption
Genetic counseling & testing 🧬
Familial CRC, influenced by genetic & environmental factors, increases CRC risk 2 – 3 folds, while Hereditary Syndromes with highly penetrant genes carry a 70 – 90% lifetime risk.
Family history & genetic testing help guide screening, surveillance & prevention
Who to refer for genetic testing?
These are individuals with:
a) Personal history of:
- CRC before age 50
- CRC and endometrial cancer at any age
- CRC and ovarian cancer at any age
- CRC and stomach, small bowel, biliary or urinary tract cancer at any age
- CRC and 2 first-degree relatives with history of colorectal, endometrial, or ovarian cancer at any age
- 10 or more adenomatous polyps
- Multiple primary colon cancers at any age
b) Family history of inherited syndromes e.g. Lynch, FAP or familial diffuse gastric cancer
c) Cumulative > 5 proximal serrated polyps, at least two > 10 mm
d) Cumulative > 10 serrated polyps
e) 2 juvenile or Peutz-Jeghers polyps
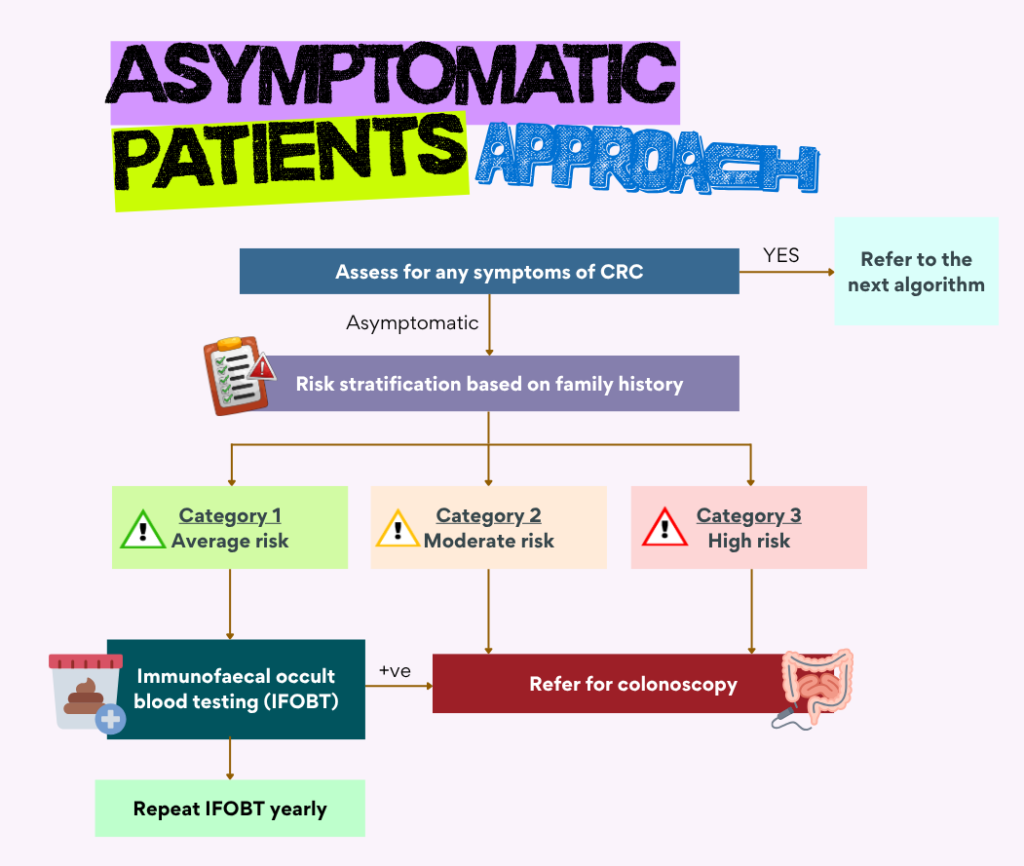
Algorithm to approach CRC screening
The approach will depends on whether the individuals are symptomatic or not
Asymptomatic
Symptomatic
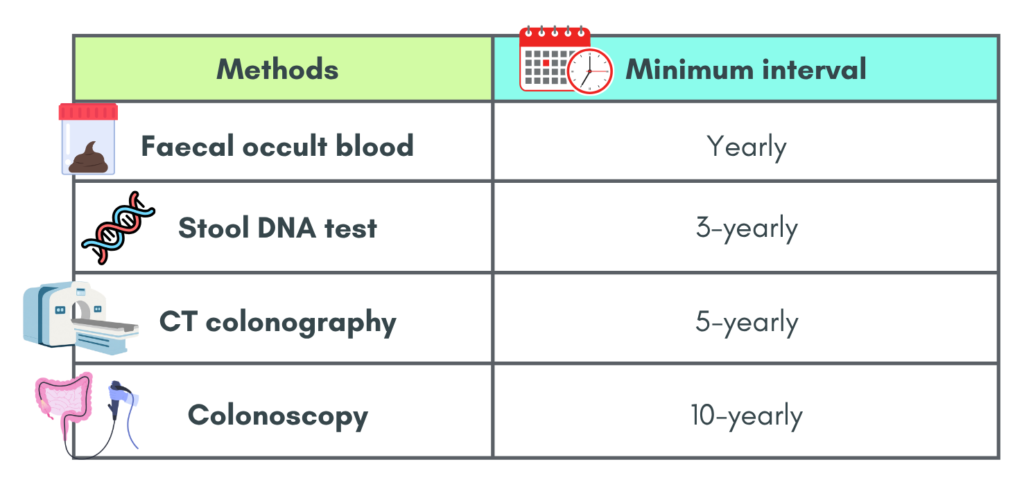
Screening interval
Below are the recommended screening intervals for CRC based on each methods
References
- Ministry of Health Malaysia. 2017. Clinical Practice Guidelines, Management of Colorectal Carcinoma.
- US Preventive Services Task Force, Davidson, K. W., Barry, M. J., Mangione, C. M., Cabana, M., Caughey, A. B., Davis, E. M., Donahue, K. E., Doubeni, C. A., Krist, A. H., Kubik, M., Li, L., Ogedegbe, G., Owens, D. K., Pbert, L., Silverstein, M., Stevermer, J., Tseng, C. W., & Wong, J. B. (2021). Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA, 325(19), 1965–1977. https://doi.org/10.1001/jama.2021.6238