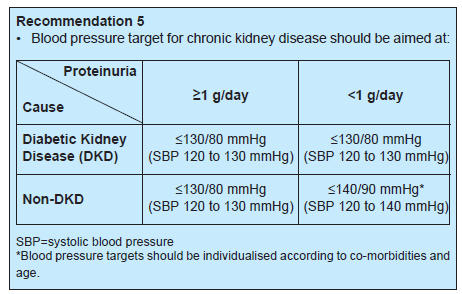
Less intensive BP lowering therapy in people with frailty, high risk of falls & fractures, very limited life expectancy or symptomatic postural hypotension
Screening for complications
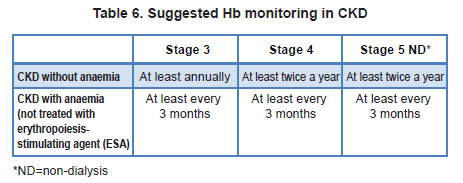
1. Anemia (usually occurs when eGFR <60)
Screening for anemia should be done when eGFR < 60.
When the eGFR is >= 60 the anemia is likely to be due to other causes.
Other causes of anemia should be excluded during the work-up for renal anemia
Treatment with ESA must be commenced by or in consultation with a nephrologist
Optimal Hb target: 10 – 12 g/dL, but should also be individualized based on symptoms and co-morbidities
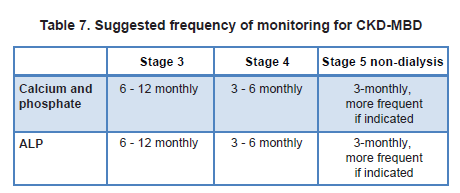
2. CKD-Mineral and Bone Disorder (CKD-BMD)
Changes in the metabolism of calcium, phosphate, PTH and ALP typically start to occur when eGFR < 60.
Screening for CKD-MBD should be done when eGFR < 45.
Elevated phosphate level should be lowered towards the normal range & hypercalcaemia should be avoided in most stages of CKD.
In hyperphosphataemia, dietary restriction of phosphate is recommended.
If persistent, dietary compliance should be re-assessed before considering the use of phosphate binders.
Excess calcium administration & vitamin D analogue should be avoided as there may be increased risk of vascular calcification in CKD.