Abnormal Uterine Bleeding
Abnormal Uterine Bleeding
Normal Menstrual Cycle
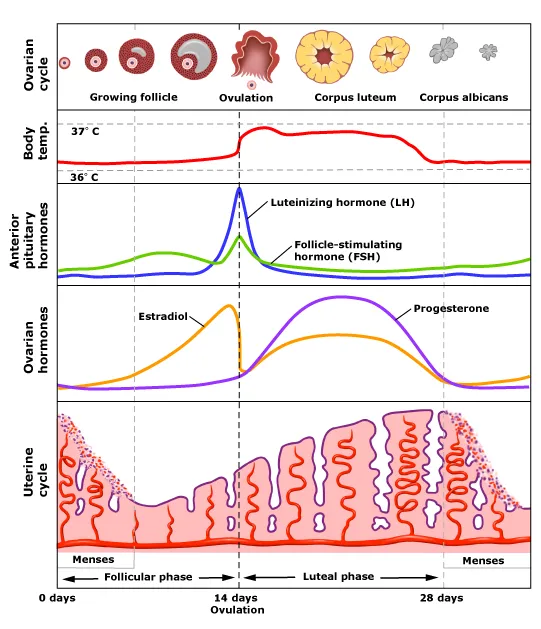
Frequency: 24 – 38 days
Flow: 2 – 7 days
Blood loss: 5 – 80 mL
Any variations are considered as AUB
FIGO classification
AUB encompasses heavy menstrual bleed (HMB), irregular cycles, disorders of cycle length and intermenstrual bleed (IMB)
Previous terminologies like menorrhagia, metrorrhagia, oligomenorrhoea, polymenorrhoea, etc. are not recommended anymore. Instead FIGO has established a more defined descriptive terms based on frequency, regularity, duration and volume of flow (FIGO AUB System 1) that is be applied across different fields including clinical practice and research studies.
FIGO AUB System 1
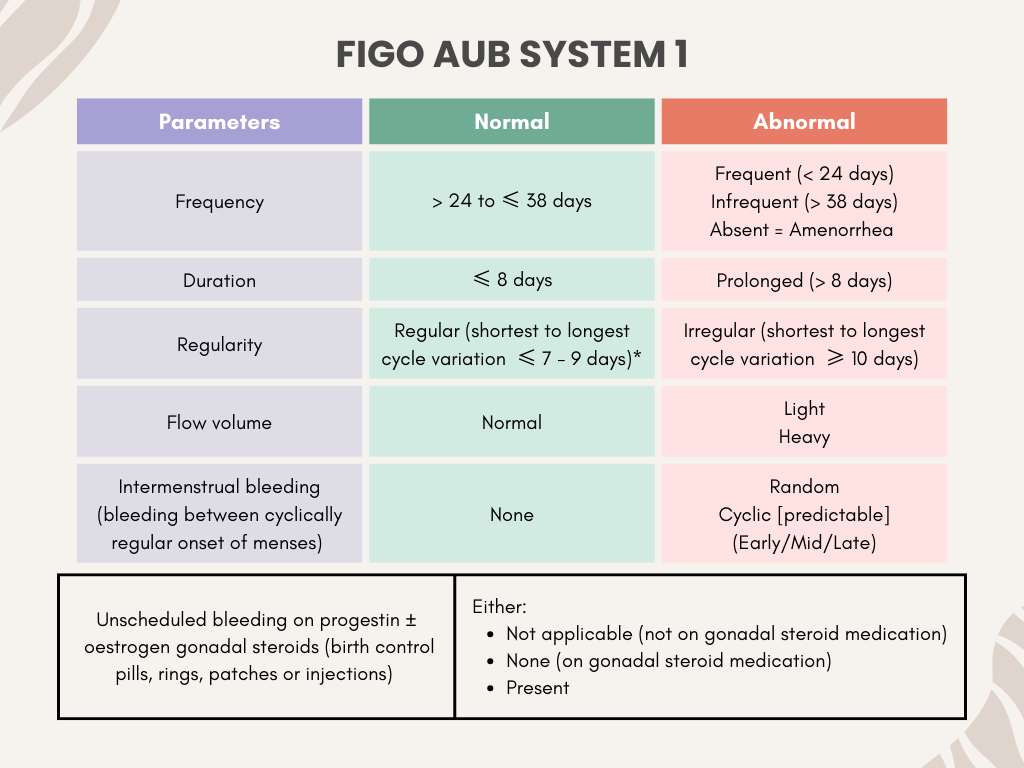
* The regularity of menstrual cycle is dependent on age, where for those aged 18 – 25 years and 42 – 45 years old, the variation can be up to 9 days. For those aged 26 – 41 years, the variation may be up to 7 days (smaller range).
The system also includes unscheduled bleeding for patients who are on hormonal medications (whether in pills/ injections/other forms of administration)
The parameters are assessed based on the cycles of previous 6 months, provided there has not been any pregnancy.
FIGO system 2 (PALM-COEIN)
Serves to categorize the possible cause of AUB into structural (“PALM”) and nonstructural (“COEI”)
The N stands for other causes that are not otherwise classified.
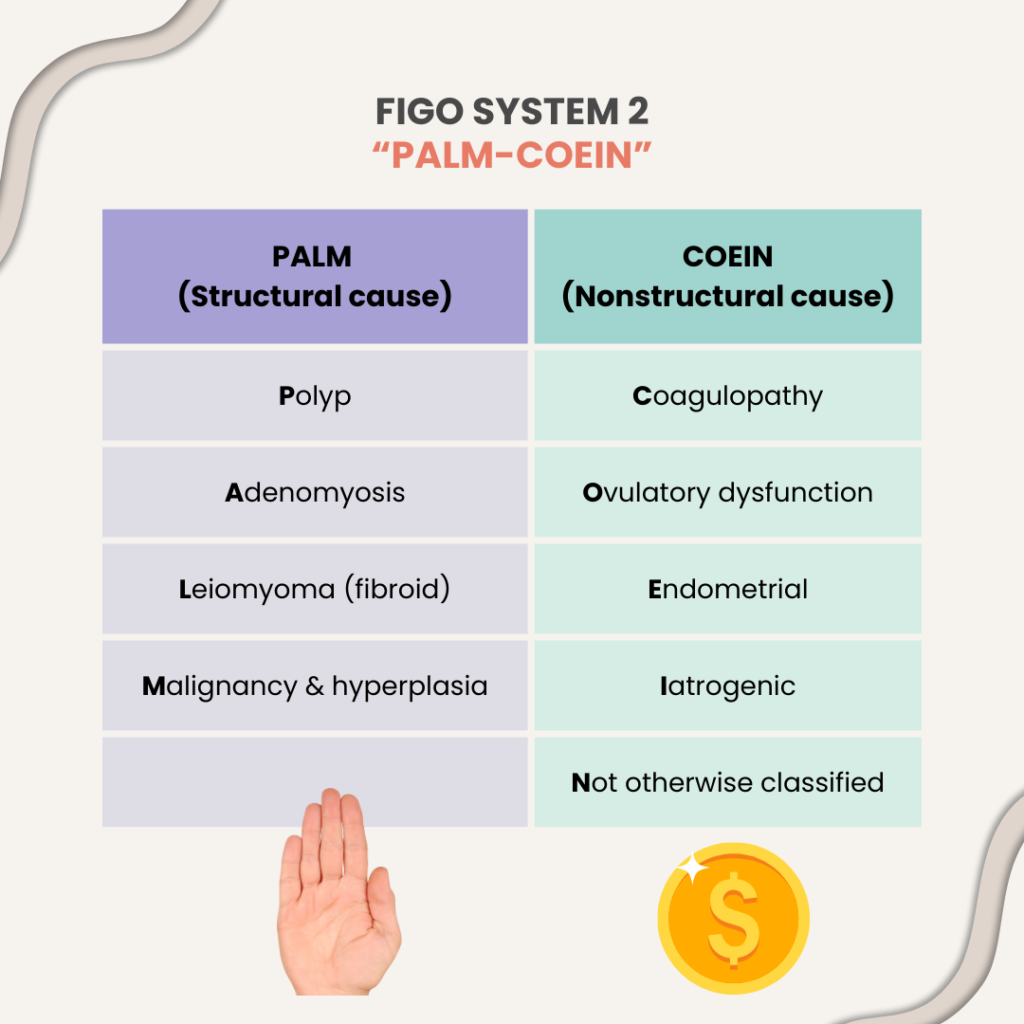
Regarding leiomyoma – FIGO has a subclassification system depending on its location (submucosal/intramural/subserosal), in which it might be good to know at primary care level. You may look up on it further if you’re interested.
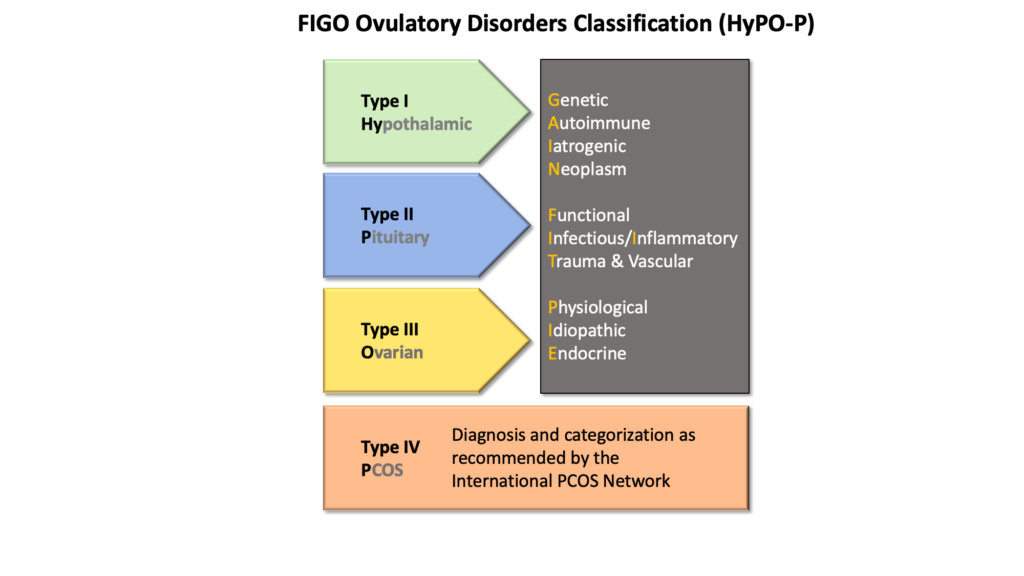
Regarding ovulatory dysfunction
- Generally suggested by h/o irregular bleeding, though it exist as a spectrum where it can also manifest as amenorrhoea or abnormalities in bleeding volume, duration and frequency
- FIGO also has a further classification for ovulatory dysfunction with the acronym “HyPO-P” to delineate the anatomical source of ovulatory dysfunction followed by the acronym “GAIN-FIT-PIE” to ascertain the probable mechanism according to the anatomical dysfunction.
Regarding coagulopathy
Screening for coagulopathy can be done by assessing for these conditions:
If HMB has been present since menarche
One of the following conditions:
- Previous postpartum hemorrhage
- Surgery-related bleeding
- Dental-related bleeding
2 or more of the following conditions:
- Frequent bruising (at least 1 – 2 times a month)
- Epistaxis (1 – 2 times a month)
- Frequent gum bleeding
- Family history of bleeding symptoms
Modified from Kouides PA, Conard J, Peyvandi F, Lukes A, Kadir R. Hemostasis and menstruation: appropriate investigation for underlying disorders of hemostasis in women with excessive menstrual bleeding. Fertil Steril 2005;84:1345–51.
Regarding Not otherwise classified – At present, includes AV malformation and caesarean scar defect.
While assessing a patient with AUB, FIGO AUB system 1 acts as a gateway to FIGO system 2.
Assessing the type of abnormalities in menstrual bleeding using FIGO system 1 can aid us in determining the probable cause of AUB using FIGO system 2 and investigate accordingly.
For example
- Heavy bleed with normal frequency and regular cycles – Differentials include coagulopathies, leiomyoma (fibroids), adenomyosis or primary endometrial disorder.
- Irregular cycles usually suggests ovulatory dysfunction
- Intermenstrual bleed – Differentials include polyps, malignancy/endometrial hyperplasia. A consistently early cycle IMB may be due to caesarean scar defect.
The diagnosis is denoted accordingly to the cause in system 2. e.g. AUB secondary to polyp is denoted as AUB-P, AUB secondary to coagulopathy is denoted as AUB-C, etc.
It is important to keep in mind that more than one causes may be present at one time.
Investigations
Investigations are individualized according to the likely aetiology and these may include:
a) UPT – whenever indicated or when pregnancy is suspected
b) Blood tests
- FBC – to look for anaemia
- Iron profile – to check for iron status/IDA (especially in HMB)
- Coagulation profile – if screening for coagulopathies is positive
- Thyroid function test – abnormal thyroid levels can also cause AUB
c) Imaging
- USG (TVS preferable or else TAS may also be used) – to assess for any structural cause
- Sonohysterography, MRI (as appropriate)
d) Endometrial sampling – if suspecting malignancy/endometrial hyperplasia
- Should be 1st line in patients > 45 years
- Should be considered in patients < 45 years old with h/o unopposed estrogen exposure (e.g. obesity, PCOS), failed medical management and persistent AUB.
e) Hysteroscopy
Management
AUB may be acute or chronic.
Acute AUB refers to heavy bleed that necessitates immediate intervention to reduce further blood loss. It may occur spontaneously or superimposed on chronic AUB ( Chronic AUB = AUB which is present for most of the previous 6 months)
When managing Acute AUB, it is important to determine the hemodynamic stability of the patient. Treatment will be based on clinical stability and suspected etiology. Often time, medical treatment is preferred although sometimes surgical intervention may be needed.
Consideration should be given for any contraindications, especially when using hormonal treatment (in accordance to the WHO medical eligibility criteria for contraceptive use)
Managing Unstable Acute AUB (without known or suspected bleeding disorders)
Set up large bore cannula with fluid resus while arranging transport to tertiary center. Manage ABCs accordingly.
Medical treatment may include:
a) Hormonal
- IV Conjugated estrogen 25 mg IV every 4 – 6 hours for 24 hours.
- 35 ug high dose COCs TDS for 7 days then OD, tapered after bleeding cessation.
- Progestin-only:
– Oral medroxyprogesterone 20 mg TDS for 7 days OR
– Norethisterone 10 – 20 mg TDS for 7 days
b) Non-hormonal
- Tranexamic acid
– IV 10 mg/kg up to 600 mg per dose OR
– PO 1.5g TDS for 5 days - NSAIDs (as adjunct)
Managing Stable Acute AUB (without known or suspected bleeding disorders)
Management is often based on suspected etiology, patient’s desire for fertility, and underlying medical problems.
Medical management is preferred and may include
a) Hormonal
- Levonorgestrel-releasing intrauterine system (LNG – IUD)
- COCPs – monophasic 30 – 35 mcg daily with or without inert pills (helps in regulating ovulatory dysfunction also)
- Progestin-only:
– Oral medryoxyprogesterone 5 – 10 mg daily
– Norethisterone 5 – 10 mg OD
b) Non-hormonal
- Tranexamic acid – PO 1.5 g TDS for 5 days
- NSAIDs – Ibuprofen (600 mg QID or 800 mg TDS), Mefenamic acid (500 mg TDS), Naproxen
Once acute AUB is controlled, long term-management/maintenance therapy can be started to reduce blood loss in future cycles depending on the suspected etiology.
COCs, oral or injectable progestins, LNG-IUDs, tranexamic acid and NSAIDs are available options.
Mentioned above are general approach to managing AUB that are more likely to be helpful in primary care setting. Nevertheless, specific etiology may have their own management guideline which may require input from relevant specialist e.g. adenomyosis, fibroids, coagulopathies etc. and will not be included in this post.
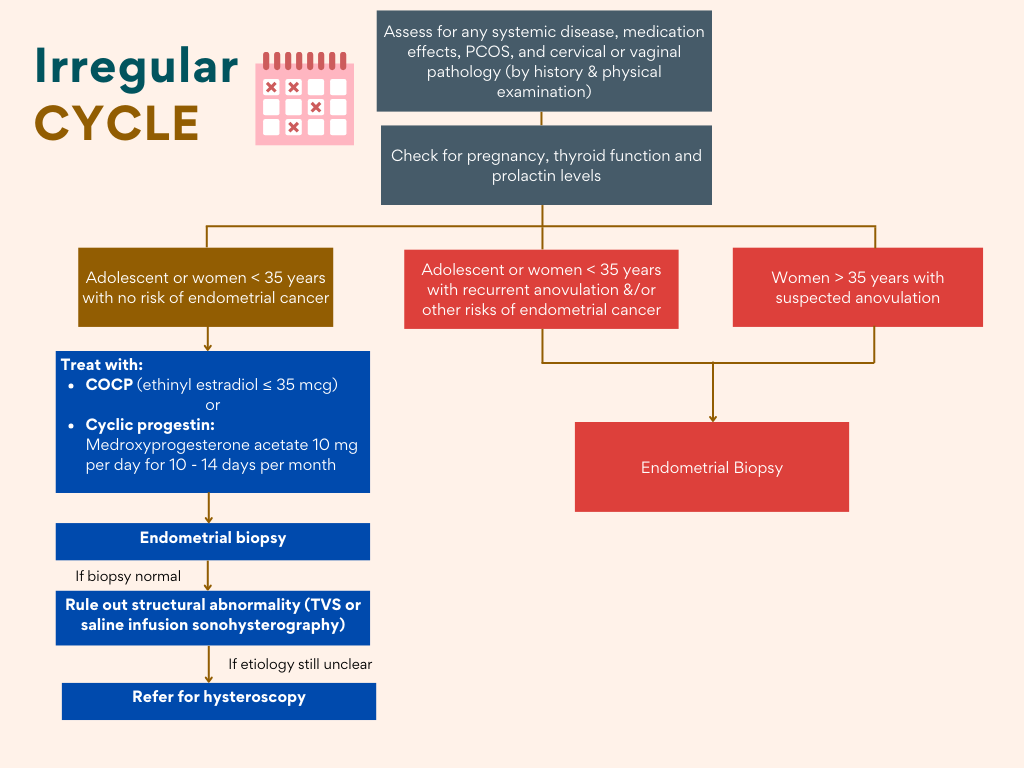
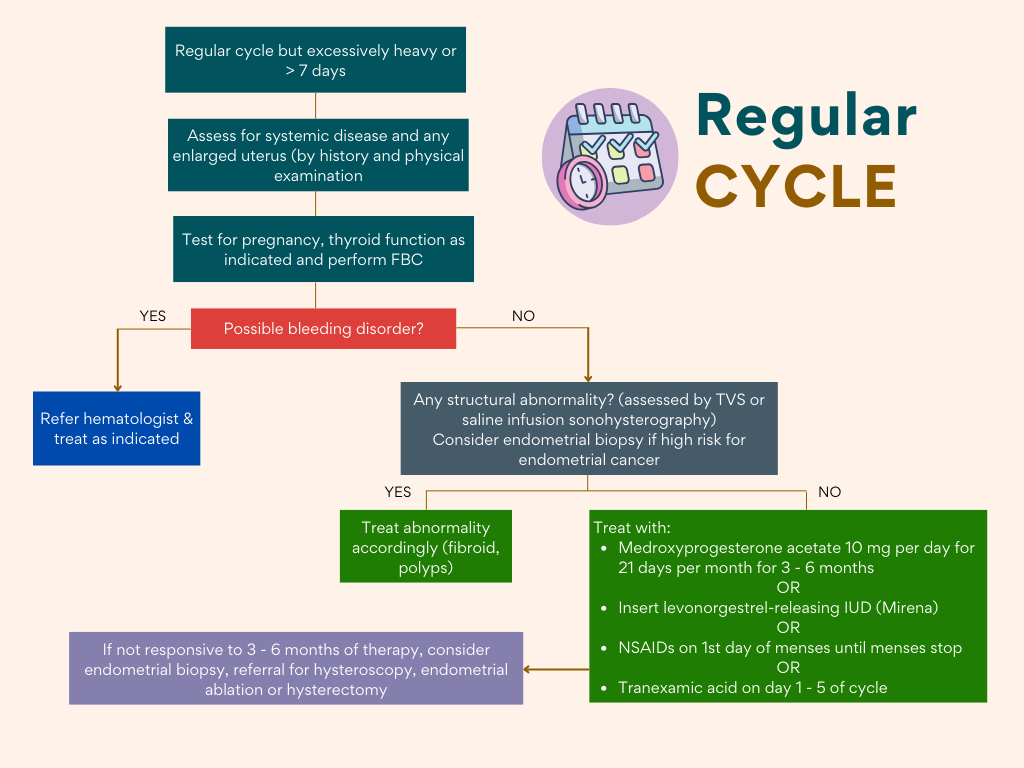
Algorithm
These algorithm may provide some useful approach to AUB in clinical practice.
Sweet, M. G., Schmidt-Dalton, T. A., Weiss, P. M., & Madsen, K. P. (2012). Evaluation and management of abnormal uterine bleeding in premenopausal women. American family physician, 85(1), 35–43.
References
- Jain V, Munro MG, Critchley HOD. Contemporary evaluation of women and girls with abnormal uterine bleeding: FIGO Systems 1 and 2. Int J Gynecol Obstet. 2023; 162(Suppl. 2): 29-42. doi:10.1002/ijgo.14946
- Mikes BA, Vadakekut ES, Sparzak PB. Abnormal Uterine Bleeding. [Updated 2025 Feb 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532913/
- Sweet, M. G., Schmidt-Dalton, T. A., Weiss, P. M., & Madsen, K. P. (2012). Evaluation and management of abnormal uterine bleeding in premenopausal women. American family physician, 85(1), 35–43.