Non-neurogenic Male LUTS
Male LUTS (non-neurogenic)
This post will be focusing on non-neurogenic male Lower Urinary Tract Symptoms (LUTS) where overactive bladder and benign prostatic enlargement will also be discuss briefly here.
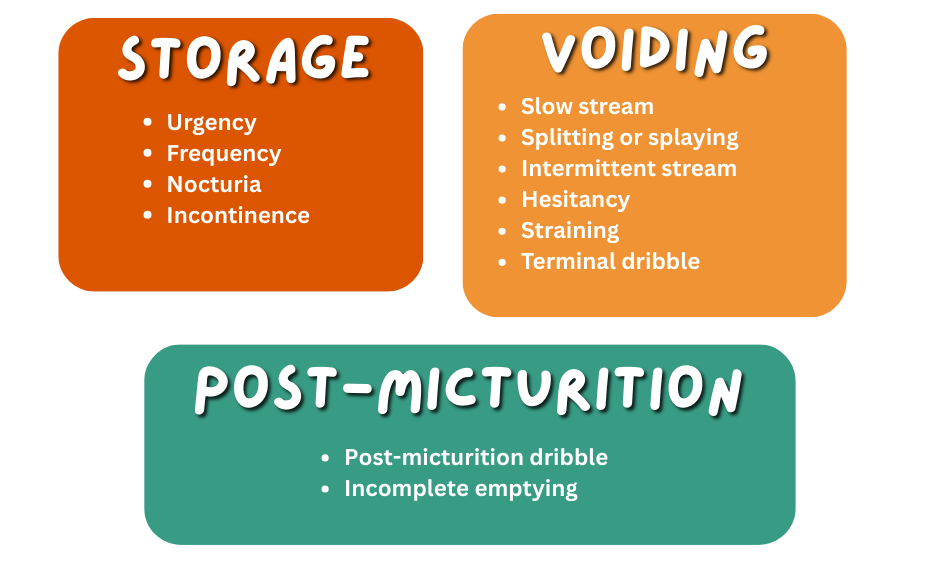
LUTS can generally be categorized into storage, voiding and even post micturition symptoms as depicted below.
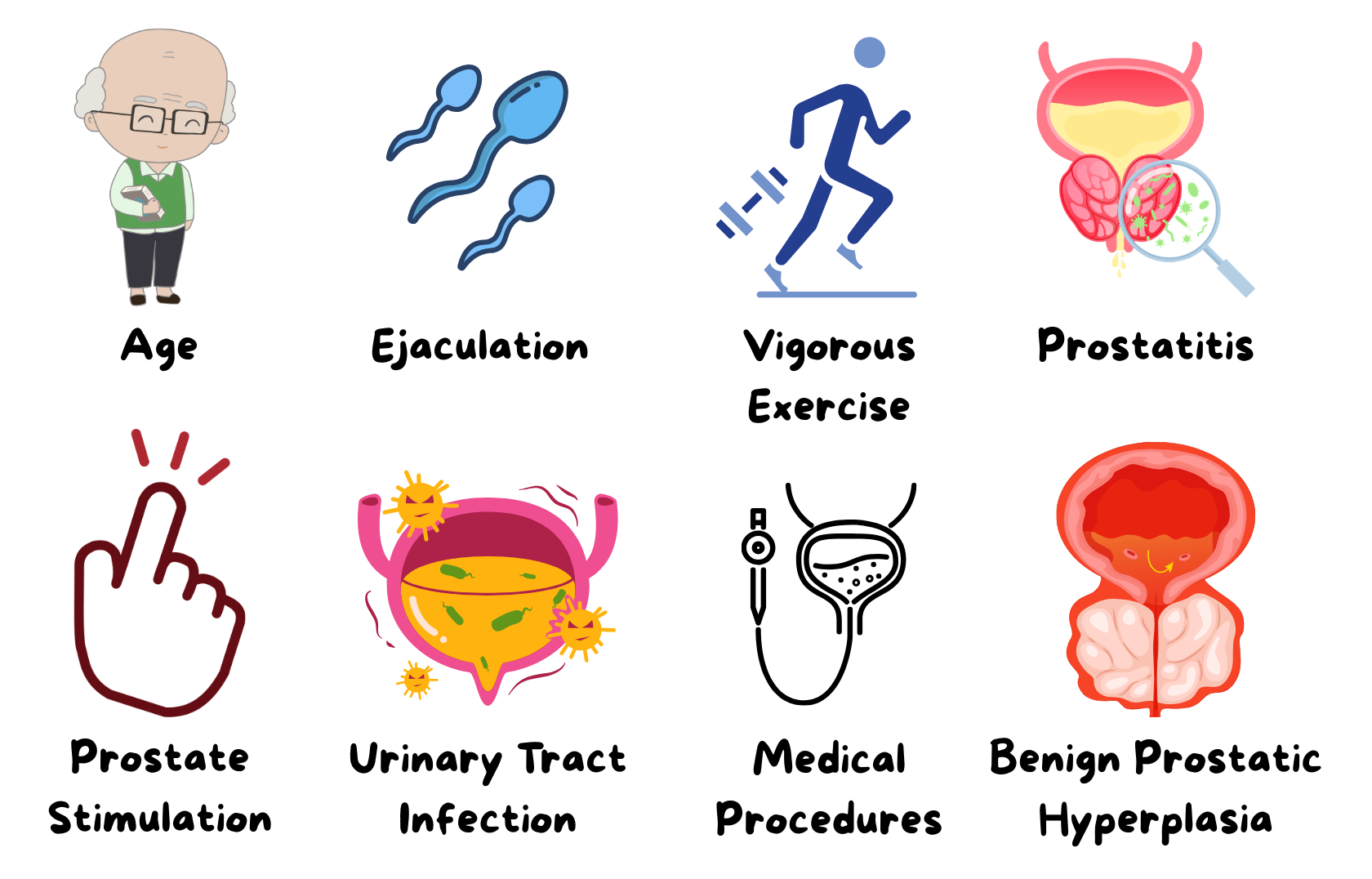
Causes
There are various causes of LUTS.
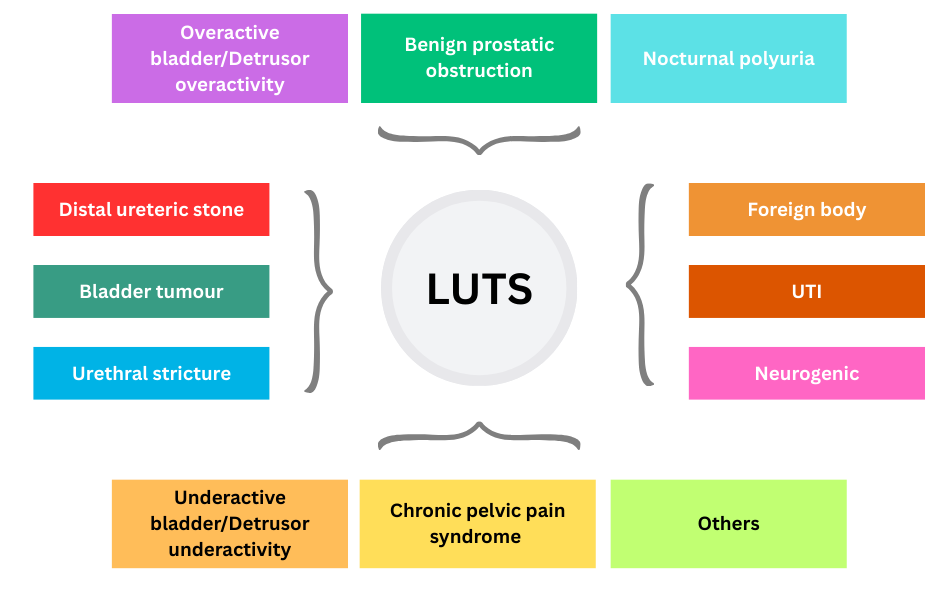
History & physical examination are important to guide us towards the various differential diagnosis.
Physical examination may include:
- General well-being
- Body habitus (obesity)
- Gait & neurology
- Abdomen – tenderness, distended bladder
- Genitalia – meatus
- DRE – prostate size, median sulcus, nodule, consistency
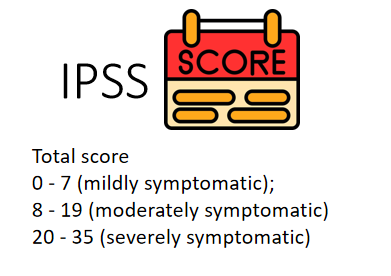
Assessing severity
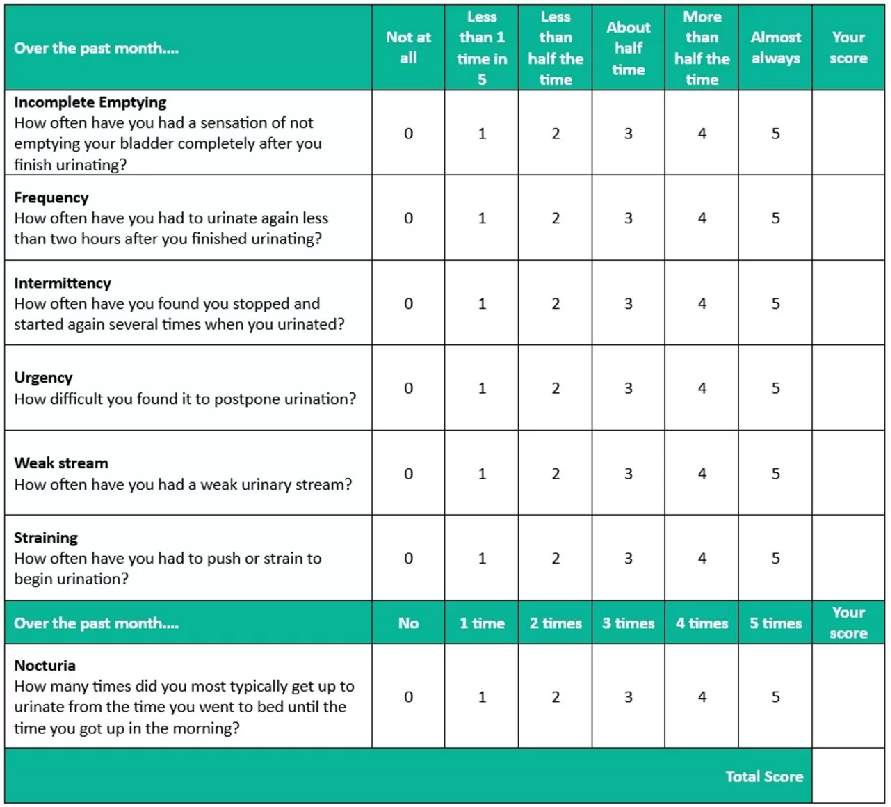
The IPSS might be a suitable tool to assess the severity of patient’s symptoms and guide treatment decision.
Investigations
Blood test to consider
- FBC
- Renal profile
- Glucose/HbA1c
- Calcium, uric acid – if suspecting calculi
- PSA (especially in elderly patients)
Regarding PSA
Has a good predictive value for assessing prostate volume & is a strong predictor of prostate growth.
Baseline PSA can predict the risk of AUR & BPO-related surgery.
EAU recommendations:
- Measure PSA if a diagnosis of prostate CA will change management
- Measure PSA if it assists in the treatment &/or decision-making process
- Counsel patients about PSA testing & the implications of a raised PSA test
Keep in mind that PSA is organ specific and not disease specific. Thus, a raised PSA does not necessarily means carcinoma
Possible causes of raised PSA
(excluding malignancy)
Urine test
- UFEME
- Culture & sensitivity if indicated
Others
- USG KUB – prostate size, bladder (trabeculations, wall thickening, calculi), hydronephrosis
(If you are interested in learning more on the role and application of USG KUB in primary care, you may consider getting a copy of this ebook here – USG at the point of care focusing on HBS & KUB, primary care perspective) - Uroflowmetry
- Cystoscopy
- Urodynamic study
The following section briefly discusses benign prostatic hyperplasia and overactive bladder, and is not intended to address every causes of LUTS.
More detailed aspect of BPH and overactive bladder will be discussed in a separate post.
A. Benign Prostatic Hyperplasia
BPH is a tissue diagnosis. (Without a tissue sample, clinically it is called as prostatic enlargement)
It is a benign, progressive enlargement of the prostate gland.
It can lead to reduced QoL & affects sexual function.
May cause urinary retention, leading to recurrent UTI, stones, CKD.
For mild or moderate symptoms
EAU recommends watchful waiting + lifestyle advice if patient is minimally bothered by their symptoms.
Behavioral & dietary modifications include:
- Education & reassurance
- Reduce fluid intake at specific time (at night)
- Avoid caffeine/alcohol
- Double voiding technique (if patient has sensation of incomplete voiding)
- Urethral milking post micturition (if patient has post void dribble)
- Bladder retraining
- Treat constipation
Pharmacological treatment 💊
Generally consist of :
- Alpha-blockers (dynamic component)
- 5-alpha reductase inhibitors (5ARI) (static component)
- Phosphodiesterase 5 inhibitors (PDE5 inhibitors) – only tadalafil 5 mg OD has been licensed for BPH treatment
- Antimuscarinic (if predominant storage symptoms)
The commonly used are the alpha-blockers and 5ARI.
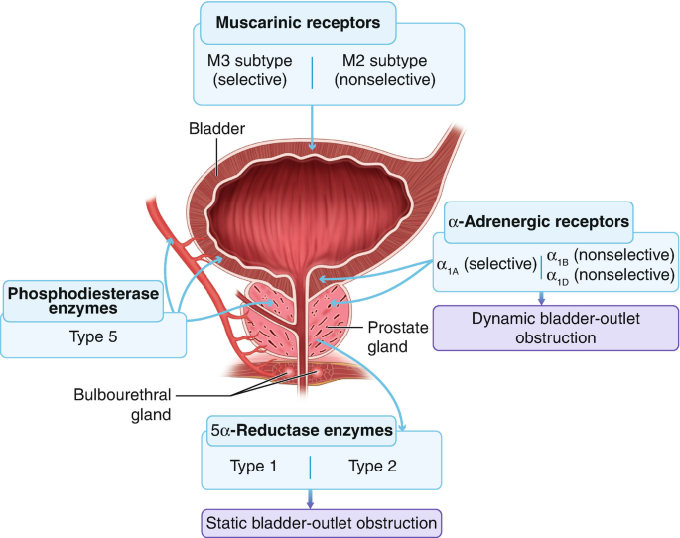
Alpha blockers
Mechanism of action: Relaxation of the prostatic stroma smooth muscles.
Examples : Tamsulosin, Silodosin, Alfuzosin, Doxazosin, Terazosin
Common adverse effects :
- Asthenia (fatigue or weakness), dizziness & postural hypotension
- Abnormal ejaculation (retrograde ejaculation/ejaculation failure)
- Intraoperative floppy iris syndrome (0.9 – 3.7%) in cataract surgery
** Does not affect libido, sexual function
5-alpha reductase inhibitor (5ARI)
Mechanism of action: Reduce conversion of testosterone to DHT –> reduce prostate size
Examples : Dutasteride, Finasteride
Consider starting in patient with prostate size > 40 mL (risk of progression)
Common adverse effects :
- Mainly affect sexual function – reduced libido, ED, ejaculation disorders, reduced semen volume, gynecomastia (1 – 2%)
Which one to start – Alpha blocker/5ARI?
Alpha blockers can be started for all patient (provided there is no contraindication and use should be caution in elderly due to risk of hypotension)
5-ARI – for patients with prostate size > 40 mL.
Combination therapy (Duodart : Tamsulosin + Dutasteride) can also be considered.
Indications for surgical intervention
- Recurrent urinary retention
- Recurrent UTI
- Bladder stone(s)
- Recurrent hematuria
- Upper urinary tract dilatation
- Renal impairment
- Non-responding to medical treatment
B. Overactive bladder
Due to detrusor overactivity
Diagnosis of exclusion
Definition :
- Urinary urgency usually with frequency & nocturia. [Note that urgency is the main complaint]
- Can be with (wet OAB) or without (dry OAB) incontinence
- Should be in the absence of UTI or other urethro-vesical pathology

Non-pharmacological management
Behavioral therapies
- Treatment of modifiable risk factors (e.g. weight reduction)
- Reduce exposure to bladder stimulants (e.g. alcohol, caffeine, smoking, carbonated beverages)
- Constipation avoidance
- Fluid optimization – restrict fluid intake to 6 – 8 glasses of water per day
Bladder training
- Develop schedule to PU
- Urinate at definite intervals (e.g. 30 mins) then increase gradually by half an hour until urinating every 3 – 4 hours.
Pharmacological management 💊
Mainstay : Antimuscarinic
Alternative : B-agonists (Mirabregon) – contraindicated in severe uncontrolled HTN (SBP ≥ 180/DBP ≥ 100)
Combination therapy if refractory to monotherapy
Others
- Intra-detrusal BOTOX injection
- Sacral neuromodulation
- Posterior tibial nerve stimulation (PTNS) – 12 sessions each lasting around 30 mins
- Last resort: augmentation cystoplasty
Simplified approach to Male LUTS
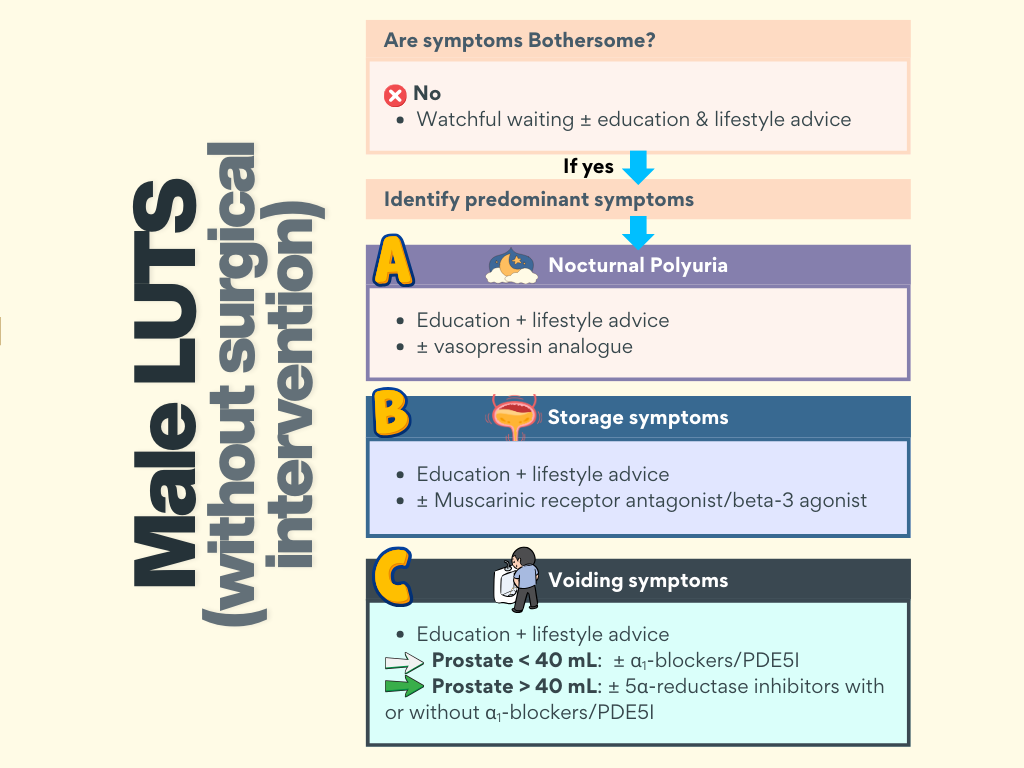
Key points
- Start treatment is symptoms are bothersome.
- Nocturnal polyuria – vasopressin
- Storage symptoms – Muscarinic receptor antagonist/β3 agonist
- Voiding symptoms
– Prostate < 40 mL – ⍺1-blockers/PDE5I
– Prostate > 40 mL – 5-ARI ± ⍺1-blockers/PDE5I
Indications for prostate surgery :
- When LUTS or post-void residual remain bothersome despite conservative or medical treatment.
- When there is upper urinary tract dilatation secondary to benign prostatic obstruction with or without renal impairment
References
- Gratzke C, Bachmann A, Descazeaud A, Drake MJ, Madersbacher S, Mamoulakis C, Oelke M, Tikkinen KAO, Gravas S. EAU Guidelines on the Assessment of Non-neurogenic Male Lower Urinary Tract Symptoms including Benign Prostatic Obstruction. Eur Urol. 2015 Jun;67(6):1099-1109. doi: 10.1016/j.eururo.2014.12.038. Epub 2015 Jan 19. PMID: 25613154.
- Docquity. Urology Masterclass – Management of Male LUTS and OAB [Webinar]