Shoulder X-ray (Trauma series)
Normal views: AP and Lateral Y view (most common)
AP view and Lateral Y view are the most commonly used.
Other views: Axial/Armpit view, Apical oblique view

This post is not a detailed cover of shoulder X-ray and all of its related fracture, but rather more on tips and points that might help you on your interpretation on Shoulder X-rays =)
Regarding dislocation
Anterior dislocation are the most common.
When there is anterior dislocation of the shoulder joint, remember to assess also for any fracture associated with impaction of the humeral head against the glenoid margin:
– Hill-Sachs deformity: Compression fracture of the posterolateral aspect of the humeral head
– Bankart’s lesion: Fracture of the anterior lip of the glenoid.
Posterior dislocation are less common and are often caused by violent muscle contraction, either during a convulsion or electric shock.
There may be associated reversed Hill-Sachs deformity and reversed Bankart’s lesion (radiopaedia). Axillary view is an alternative view.
Dislocation can and should be assessed in both AP and lateral Y view.
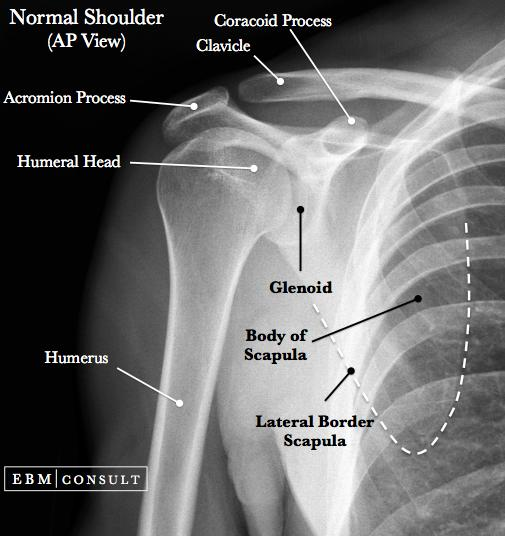
AP view
Anterior dislocation – humeral head seen outside of the glenohumeral joint and may lie beneath the coracoid process.
Posterior dislocation – may be missed in AP view as the humeral head appears within the glenohumeral joint. The humeral head often have a rounded appearance (due to fixed internal rotation) which may look like a light bulb (light bulb sign).
Anterior dislocation: humeral head lies outside the glenohumeral joint and beneath the coracoid process.

Posterior dislocation: humeral head appears rounded and has a “light bulb” appearance
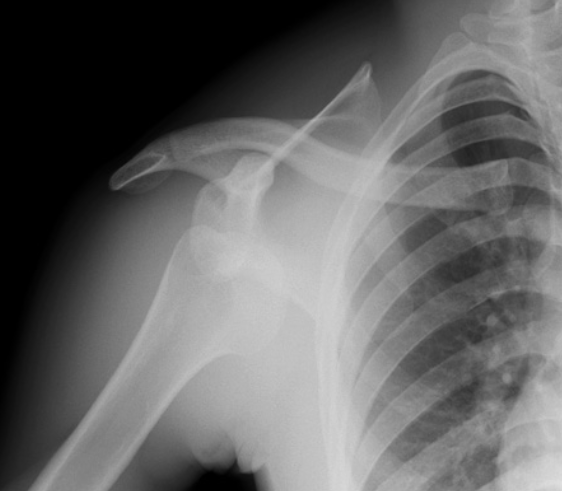
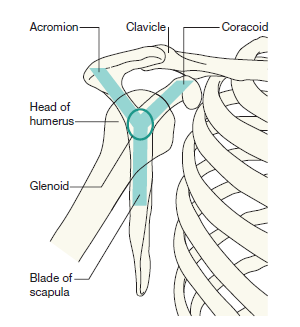
In lateral Y view, dislocation can be assessed by looking at the area where the 3 lines intersect (center of the “Y”). In a normal shoulder joint, the humeral head lies over the center of the “Y”.
In anterior dislocation, the humeral head lies anteriorly to the “Y”; whereas in posterior dislocation, the humeral head lies posteriorly to the “Y”.

Anterior dislocation: humeral head lies anteriorly to the “Y” (towards the ribs)
Posterior dislocation: humeral head lies posteriorly to the “Y” (away from the ribs)
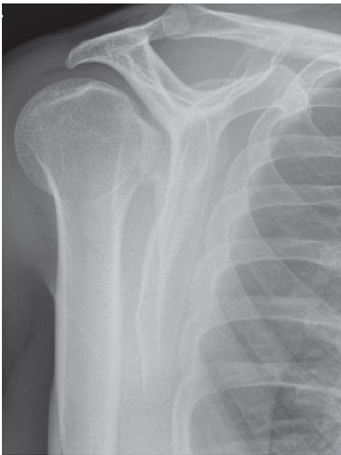
Remember to look at the acromioclavicular joint (ACJ)
In trauma setting, there may be stretching/rupture of the acromioclavicular and/or coracoclavicular ligaments leading to disruption of the ACJ.
Clues pointing to ACJ disruption:
– Inferior cortices of the clavicle and acromion do not align.
– Acromioclavicular (AC) distance > 8 mm
– Coracoclavicular (CC) distance > 1.3 cm
(Note: There may be variation of the CC distance in different individuals, comparison with the contralateral side may be more useful than the absolute value itself. There should no be more than 5 mm difference between both sides in a normal ACJ)
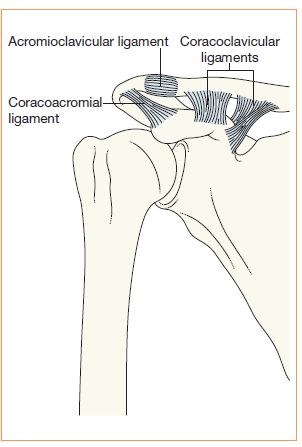
Ligaments supporting the ACJ

Rockwood classification of AC joint disruption
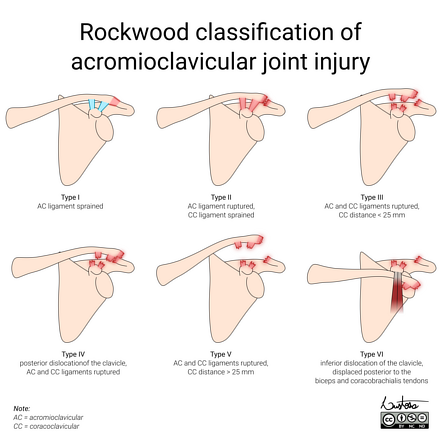
- Type I: Normal radiographic appearance
- Type II: Widened ACJ (> 7 mm) with < 25% clavicular elevation
- Type III: Clavicle elevated above the superior border of the acromion but the CC distance is less than twice normal (i.e. <25 mm) or 5mm greater than this distance on the contralateral side
- Type IV: Clavicle displaced posteriorly
- Type V: Clavicle is markedly elevated and coracoclavicular distance is more than double normal (i.e. >25 mm) – bilateral weight-bearing projections are able to distinguish type V injuries
- Type VI: Inferior displacement of clavicle
Last but not least!
Always assess the lungs and ribs while reviewing X-ray of the shoulder.
Look out for any pneumothorax, hemothorax, rib fractures, lung contusions (especially in trauma setting ) or sometimes you may even have an incidental finding of a lung tumor!